





1. Background
Advanced kidney failure is a chronic disease that requires long-term treatment methods such as dialysis or kidney transplants. While a kidney transplant is the optimal treatment method, hemodialysis is the most commonly used approach (1, 2).
The global prevalence of advanced kidney failure currently stands at 242 cases per 1 million people, with an annual increase rate of 8% (3). According to statistics, approximately 1200 to 1600 people in Iran are diagnosed with this disease each year (4). In 2013, the Head of the Transplantation and Special Diseases Department at the Ministry of Health and Medical Education reported that 32,686 kidney patients had been identified in Iran, highlighting the need to double the number of dialysis beds (5).
Hemodialysis can lead to numerous complications, including gastrointestinal issues like anorexia and anemia, neurological problems, and reproductive system complications, such as alterations in menstrual cycles. These complications disrupt patients' quality of life and may lead to depression and, in some cases, even suicide (6, 7).
Furthermore, although hemodialysis extends patients' lifespans, it introduces various challenges to their lifestyle, resulting in anxiety and stress that negatively impact their quality of life. Addressing patients' problems is always a top priority for health care systems and an essential aspect of nursing to provide appropriate care to patients (8).
A low quality of life can lead to emotional exhaustion, job loss, reduced productivity, mental health issues like depression and anxiety, and decreased physical performance (9, 10). Measuring the quality of life helps nurses provide proper care to individuals whose quality of life is significantly and irreversibly affected due to compromised functional integrity (11). Several factors influence the quality of life and its dimensions, with lifestyle being considered one of the most influential factors (12).
Lifestyle encompasses the normal and routine daily activities that people engage in throughout their lives. These activities have the potential to significantly impact an individual's overall health (12). Modifying one's lifestyle involves changing behaviors that constitute a significant part of their daily routines. If lifestyle changes do not lead to an improvement in an individual's overall quality of life, motivating them to make these changes becomes much more challenging. Numerous studies have explored the relationship between lifestyle and quality of life, examining various dimensions (13, 14). Providing patients with instructions aimed at improving their lifestyles is an effective method that offers opportunities for patients to learn about their conditions and enhance their coping mechanisms and skills (15, 16).
The Knowledge, Attitude, and Practice (KAP) model is considered one of the fundamental models for changing human behavior. This model posits that knowledge is a crucial factor in altering people's behavior, and individuals can exhibit desirable behavior by acquiring knowledge and skills (17). The Information-Knowledge-Attitude-Practice (IKAP) theory has been successfully applied in nursing care for patients with conditions such as acute pancreatitis, primary hypertension, bladder perfusion, and coronary artery disease, yielding positive outcomes (18-21).
A study demonstrated a significant improvement in the quality of life dimensions of patients with chronic obstructive pulmonary disease (COPD) 3 months after the intervention (18). Another study conducted in China focused on the impact of the IKAP theory on the motor performance of patients with cardiovascular disease. The results indicated a statistically significant difference between the control and experimental groups (21).
Chronic diseases affect individuals, families, and society in terms of economic, financial, social, and emotional well-being. Treating chronic patients goes beyond medical treatment and disease management. Research has consistently affirmed the vital role of patient education and instruction on health-related issues and the advantages of continuous nursing care based on the IKAP theory in enhancing patients' self-responsibility and independence in meeting their personal needs. However, to our knowledge, the impact of continuous nursing care based on the IKAP theory on patients undergoing hemodialysis treatment has not yet been investigated. To date, the use of this safe and cost-effective educational model in patients with chronic diseases has yielded positive results.
2. Objectives
This study aimed to determine the effect of the IKAP theory on continuous nursing care and the quality of life of patients undergoing hemodialysis treatment.
3. Methods
3.1. Study Design, Setting, and Definitions
This interventional study with a comparison group was conducted using 2 parallel groups at Sina and Imam Khomeini university hospitals in Ahvaz from October 2021 to February 2022. The sample was selected based on the following inclusion criteria: Willingness to participate in the research, the ability to read and write, the possibility of direct phone calls with the patient and an active family member, the ability to complete the questionnaire, and participation in interviews no history of mental illness or hospitalization in a psychiatric hospital Exclusion criteria included the following: The patient's death during the study, the emergence of new physical problems that hindered their ability to care for themselves and continue the training process, and the patient's unwillingness to cooperate with the researcher throughout the study.
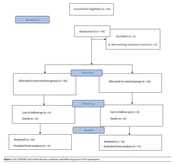
With α = 0.05, β = 0.1, and utilizing SGRQ Score information from Li et al.'s study (18), the sample size was calculated using the following formula, resulting in 56 people. The final sample size for each group was set at 34 people, totaling 68 people, accounting for a 10% attrition. This is shown in Figure 1.

The CONSORT chart of the selection, evaluation, and follow-up process of the participants
After obtaining informed consent and explaining the research objectives to the participants, they were randomly categorized into 2 groups: The experimental and control groups. Randomization was conducted using a random number table, which means that patients with odd individual file numbers were assigned to the control group, while those with even file numbers were assigned to the experimental group. The patients were scheduled to visit hospitals on either odd or even days to ensure that the 2 groups did not have contact,
At the beginning of the study, both groups completed demographic, lifestyle, and quality of life questionnaires. While the control group received routine care, including verbal training related to the disease and care, as well as educational pamphlets, the experimental group received an additional 20 to 30 minutes of continuous nursing care based on the IKAP theory every 2 weeks, in addition to routine care.
Initially, a briefing session was conducted with several objectives: To introduce the researcher to the patients and 1 of their active family members involved in their care, to provide essential information about the specifics of the disease, to identify problems accurately, to recognize the possibilities and limitations, to motivate participants according to their follow-up needs, to define their expectations from each other, and to involve the patients in the development of continuous care behaviors to the extent possible. During this stage, the researcher identified and documented their educational needs through discussions with the patients and their families, allowing for the preparation of educational content based on these needs for the implementation phase. Subsequently, following prior phone arrangements, a 30 - 45-minute session was scheduled with the researcher and each patient in attendance. During this session, participants and the researcher agreed on goals, modes of communication, and suitable times for face-to-face meetings or telephone contacts. They also expressed their expectations from the program and emphasized the importance of maintaining therapeutic relationships. The date of the next meeting was announced at the conclusion of the session.
Given that the researcher provided training to the patients in this study, it was not possible to blind the patients and the researcher, and therefore, blinding was not implemented.
The sessions were initially led by 1 of the researchers in a question-and-answer format, followed by the presentation of instructional material. At the end of each session, patients received an educational pamphlet and were asked questions related to the topics covered in the previous session. Information collection took approximately 15 minutes, knowledge acquisition took 10 - 15 minutes, and changes in patients' views and performance were evaluated after the intervention. Information was collected and analyzed 1 month and 3 months after the intervention. In this study, considering the importance of providing specialized training, routine care, and continuous nursing care consistent with the IKAP theory was delivered by 1 of the researchers, with the collaboration of several trained healthcare providers, including 1 psychiatric nurse, 1 nutritionist, and 2 clinical nurses. These providers received group training in a face-to-face format over 3 sessions. The content and presenter of each session are outlined in Table 1.
| Session | Content | Presenter |
|---|---|---|
| First | Based on research objectives, the concepts, importance, and benefits of IKAP continuous nursing care were taught. | Clinical nurse |
| Second | Based on the content of the quality of life and lifestyle questionnaire, the participants were taught about hemodialysis, amount of exercise, emotional and physical health, restriction of fluid intake, sleep pattern, and physical and sexual activities. | Clinical nurse; psychiatric nurse |
| Third | Stress management, the kind of nutrition, and exercise were instructed. | Clinical nurse; psychiatric nurse; nutritionist |
| Fourth | The researcher encouraged the patients to develop habits that would protect and improve their health. This involved using individual intervention measures for patients, helping them gain a proper understanding of their disease, preparing them ideologically to understand care, ensuring their ability to consciously implement the health education program, conducting periodic examinations, assisting them in maintaining a positive mental outlook and facilitating changes in their health behavior to ultimately improve their overall health. | Clinical nurse |
The content of the training sessions was prepared based on a literature review (22-24) and was approved by 4 hemodialysis nurses and a nephrologist.
3.2. Data Collection
Data gathering was conducted using 2 questionnaires:
3.2.1. Demographic Information Questionnaire
This questionnaire gathered the personal and demographic characteristics of the respondents, including age, sex, marital status, and educational level.
Health Promoting Lifestyle Profile: Developed by Walker et al. in 1987, this questionnaire consists of 52 items in its English version, which are answered using a 4-point response format. It assesses health-promoting behaviors across 6 dimensions: Nutrition (6 questions, evaluating food patterns and food choices), exercise (5 questions, assessing regular exercise patterns), responsibility for health (10 questions), stress management (7 questions, addressing stress sources and management measures), interpersonal support (7 questions, focusing on maintaining relationships with a sense of closeness), and self-actualization (13 questions, measuring a sense of purpose, personal development, self-awareness, and satisfaction). Each question is rated on a 4-point Likert scale (1 = never, 2 = sometimes, 3 = usually, 4 = always). The overall lifestyle score falls within the range of 52 to 208. Scores below the average (130 points) indicate an undesirable lifestyle, while scores above the average signify a desirable lifestyle. In Walker et al.'s (1987) research, Cronbach's alpha coefficient for the overall score of this questionnaire was reported as 94%, and for the 6 subscales, it ranged between 88% and 90% (25). The Persian validation of this questionnaire, conducted by Mohammadi Zaidi et al., reported a Cronbach's alpha coefficient of 82% for the entire scale and between 64% and 91% for the subscales (26).
3.2.2. Kidney Disease Quality of Life Questionnaire-Short Form (KDQOL-SF)
Developed by Hays et al. (27) in 1994, this standardized self-report instrument comprises 8 health-related quality-of-life subscales and 11 kidney disease-specific quality-of-life subscales. The questionnaire includes the following dimensions: Physical performance (10 questions), role limitation due to physical problems (4 questions), role limitation due to emotional problems (3 questions), social function (2 questions), emotional well-being (5 questions), pain (2 questions), fatigue and energy (4 questions), understanding of general health (5 questions), and a general question about personal health.
The results from this tool are summarized into 2 sections, representing the components of physical and mental health status. The second part assesses kidney disease-specific factors for patients undergoing hemodialysis and includes subscales related to existing symptoms and problems, including muscle pain and chest pain (12 questions), impact of kidney disease on life (8 questions), burden of responsibility of kidney disease (4 questions), job status (2 questions), cognitive function (3 questions), quality of social interaction (3 questions), sexual function (2 questions), sleep (4 questions), social support (2 questions), encouragement by dialysis ward staff (2 questions), patient satisfaction (1 question).
A score of 100 - 76 indicates a good quality of life, 46 - 75 indicates an average quality of life, and 1 - 45 indicates a poor quality of life (27, 28). In Yekaninejad et al.'s study, the scales' validity by Cronbach's alpha was reported to be between 0.73 and 0.93 (29).
3.3. Statistical Analysis
To analyze the collected data statistically, we used SPSS v. 25.0 (Armonk, NY: IBM Corp). We conducted the Shapiro-Wilk test to assess data distribution. Baseline variables were compared between groups using the independent t-test for continuous data and the chi-square test for categorical data. Categorical variables were presented as frequencies, while mean and standard deviation (SD) were reported for continuous variables. We performed a 2 × 3 (group × time) repeated measures analysis of variance (ANOVA) to compare differences within and between groups. The time variables included baseline, 1 month, and 3 months following the intervention, and the group variables were experimental and control groups. A P-value below 0.05 was considered statistically significant.
4. Results
4.1. Patient Characteristics and Clinical Data
In this study, we did not experience any sample loss, and statistical analysis was conducted on 68 hemodialysis patients.
According to the study results, the mean and SD of the patient's age in the experimental group were 53.11 ± 11.16, while in the control group, they were 52.16 ± 9.84. The independent t-test (Table 2) did not reveal a significant difference between the 2 groups in terms of age (P < 0.397).
The chi-square test results demonstrated that the intervention and control groups were homogenous in terms of sex, education, and marital status. Regarding gender, the majority of participants were women. In terms of education, most patients held post-graduate degrees, and the majority were married (Table 3).
| Variables | Experimental Group | Control Group | P-Value b |
|---|---|---|---|
| Sex | 0.804 | ||
| Male | 13 (38.2) | 14 (41.2) | |
| Female | 21 (61.8) | 20 (58.8) | |
| Education level | 0.633 | ||
| Below high school diploma | 8 (23.5) | 8 (23.5) | |
| High school diploma | 5 (14.7) | 9 (26.6) | |
| Associate degree | 14 (41.2) | 6 (17.6) | |
| Bachelor's degree | 6 (17.6) | 2 (5.8) | |
| Marital status | 0.161 | ||
| Single | 6 (17.6) | 11 (32.4) | |
| Married | 28 (82.4) | 23 (67.6) |
a Values are expressed as No. (%).
b Chi-square test.
Regarding the results of the repeated measures test, the mean score of the overall quality of life in the experimental group showed a statistically significant difference before and after the intervention (P < 0.001). However, in the control group, this difference was not significant (P = 0.807). The results of the independent t-test, based on the within-group comparison of the mean quality of life scores, indicated that there was no statistically significant difference between the experimental and control groups before the intervention (P = 0.781). However, 1 month after the intervention, a significant difference was observed (P = 0.013), and 3 months after the intervention, the difference remained significant (P = 0.001) (Table 4).
a Values are expressed as mean ± SD.
b Repeated measurement.
c Independent t-test.
a Values are expressed as mean ± SD.
b Repeated measurement.
c Independent t-test.
Furthermore, based on the results of the repeated measures test, the mean score of lifestyle in the experimental group showed a statistically significant improvement before and after the intervention (P < 0.001). However, in the control group, the difference was not significant (P = 0.991). According to the obtained results of the independent t-test and the within-group comparison of the lifestyle mean scores, there was no statistically significant difference between the 2 participating groups before the intervention (P = 0.423). However, 1 month after the intervention, a significant difference emerged (P = 0.012). Three months after the intervention (Table 5), the difference between the experimental and control groups remained significant (P = 0.001).
5. Discussion
The present study aimed to investigate the impacts of continuous nursing care according to the IKAP model on the quality of life and lifestyle of patients undergoing hemodialysis treatment.
The results demonstrated that the quality of life mean score in the experimental group significantly increased compared to the control group after the implementation of nursing care in line with the IKAP model. In other words, continuous nursing care improved the overall quality of life of hemodialysis patients. The implementation of continuous nursing care allowed nurses to acquire essential care skills during the training phase, enabling them to execute nursing procedures correctly. These positive changes subsequently enhanced clinical outcomes and improved patients' caring behaviors, which had a positive impact on their quality of life.
It should be noted that one of the main challenges faced by patients with kidney failure is learning about treatment procedures and how to live with the disease. Therefore, implementing correct nursing care and educating patients with the aim of empowering them with self-care skills to improve their quality of life is considered an important health indicator (11, 12). Many studies have reported that patients often struggle to implement proper medical care and have emphasized the significant role of knowledge and attitude in providing optimal care to patients at the standard level (30, 31). In this study, after receiving sufficient instruction about kidney failure, its complications, and treatment compliance, nurses were able to provide optimal care to patients. This step laid the foundation for improving the quality of life of the patients.
Alikari et al. conducted a study to investigate the effect of education on awareness, adherence to treatment, and quality of life in hemodialysis patients. The analysis of the results showed that proper training in hemodialysis departments could improve the level of liveliness, general health, physical performance, mental health, and overall understanding of health, consequently increasing the overall quality of life in hemodialysis patients (32). Li et al. conducted a study with the aim of investigating the impact of continuous nursing care according to IKAP on the quality of life of patients with COPD in China. The research findings showed that all dimensions of quality of life significantly improved in patients with COPD 3 months after the intervention (18).
The results reported by Darvishi et al. on the effect of implementing the empowerment program on the quality of life of hemodialysis patients (33) and Motaghi and Zarei on the effect of using the synergy care model on the quality of life of hemodialysis patients also showed that all dimensions of quality of life significantly improved (34). It appears that nursing care measures involving patient education, the development of patient-administered self-care, and continuous follow-ups and evaluations contribute to improvements in quality of life and a reduction in mortality. Importantly, the research indicates that despite the presence of comprehensive interventions by multiple specialties, nursing intervention still has a positive effect.
The results of the current research demonstrated that the mean lifestyle score in the experimental group significantly increased compared to the control group after the implementation of continuous nursing care based on the IKAP theory. The findings of Jafari and Ghaibizadeh showed that education based on the behavioral model improved the lifestyle of hemodialysis patients (35). Additionally, Oshvandi et al.'s study showed that the implementation of an educational program improved the lifestyle of hemodialysis patients (36), which is consistent with the present study.
In fact, the establishment of regular and continuous educational programs has an impact on many aspects of the lifestyle of kidney patients, improving their behaviors and lifestyle choices. The correct choice empowers them to adopt healthy behaviors and, as a result, lead a healthier lifestyle.
Conversely, Liu et al. arrived at different results. Their study aimed to test the use of a Knowledge-Attitude-Behavior training program on the lifestyle of adults undergoing maintenance hemodialysis. The findings showed that following a training program, no significant difference was found in the overall mean score for lifestyle (37). This inconsistency with the results of this study may be attributed to different approaches to instructing patients. In Liu et al.'s study, in addition to face-to-face training, film screening was also used, whereas in the present study, nurses received face-to-face training, and the researcher and trained nurses provided nursing care based on the IKAP theory and routine care for hemodialysis patients.
Among the strengths of this study is the implementation of this model for the first time in patients undergoing hemodialysis. By using this model, nurses took an effective step in reducing the stress and physical, mental, and psychological symptoms resulting from the disease, which consequently improved the quality of life and the lifestyle of hemodialysis patients. Furthermore, the sample size and the number of hospitals for sampling were suitable.
5.1. Limitations
Regarding the limitations of this study, the patients were only followed up by phone for the implementation of the IKAP model at home for 1 month and 3 months, which is one of the limitations of this study. It would have been better if the follow-up period were longer and if the participants' previous knowledge and experiences, as well as their emotional, psychological characteristics, and cultural background, which may have impacted their learning performance and the care provided by the nurse, were considered.
5.2. Conclusions
In general, based on the results of the present study and similar research mentioned above, it can be concluded that if the goals and care plans aim to improve the patients' awareness, attitude, and practice, an increase in the level of a healthy lifestyle and the quality of life in patients can be observed. Therefore, considering the effectiveness of the IKAP theory in the training of nurses, nursing managers and policy-makers can design appropriate training programs to improve nurses' knowledge, attitude, and practice. Nurses with higher knowledge and skills can effectively convince patients to cooperate and continue to attend training programs.
Moreover, there is a limited number of research studies about the application of the IKAP theory on chronic diseases. Therefore, it would be beneficial for other researchers to investigate the application of IKAP theories in diseases such as various types of cancer, heart disease, and so on.
