1. Background
Hypertension is one of the most common, chronic, recurrent, and underlie for other diseases that can be prevented in the present age. It is considered to be a challenging medical condition due to extensive and prolonged changes in lifestyle behaviors. Despite the fact that high blood pressure can be easily diagnosed and usually easily treatable, it can often lead to fatal complications if not timely diagnosed (1). Hypertension is one of the most important factors of heart diseases (2, 3) and one of the most serious psycho-physiological disorders (4). The prevalence of this optional mute is 9.22% in developed countries; while in developing countries, this number is 22.9% (3). Genetic factors (family history), environmental factors (salt consumption, obesity, and alcohol), psychological factors (coping with stress, self-confidence), and social factors (jobs, income level) are effective in creating hypertension (5).
Emotion cognitive regulation is one of the most important factors in hypertension. People apply different emotion regulation strategies that can be adaptive or maladaptive (5). Citations of the research suggest that alexithymia is associated with difficulty in expression of emotion as well as physical health and essential hypertension (6). According to the theory of incondite, inappropriate regulation of excitement associates with autonomic nervous system incondite or continuous activation of the sympathetic nervous system, which is a direct consequence of cardiovascular disease (7). Emotion regulation strategies include nine different cognitive coping strategies (self-blame, acceptance, rumination, positive refocusing, refocus on planning, positive reappraisal, putting into perspective, catastrophizing, and other-blame) (8). The research results suggest that people with hypertension use ineffective emotion cognitive regulation strategies (9). Emotions help determine the way of life, cause a warning system when threatening, and also establish experiences to strengthen behaviors. Emotions may direct people to close or get away from a position (10).
Pickering (11) believes that pharmacotherapy is the main point of support for treating people with hypertension; however, many anti-hypertension drugs have side effects such as vertigo, headache, fatigue, and pain in chest. The side effects cause ignoring treatment by patients. Meanwhile, effective and safe anti-drug approaches for hypertension are common. Therefore, using anti-drug approaches as well as drug treatment have been considered by emphasizing the interaction between the factors to treat hypertension. Drug and non-drug methods have been used to treat hypertension. Diuretics and beta blockers are used in drug treatment. The drugs cause side effects such as reducing potassium and increasing glucose and sodium. Another weakness along with drug treatment is that by reducing orthostatic hypertension, mild digestive disorders have been reported, as well as decreasing sexual ability, gout, and increasing plasma cholesterol. On the other hand the most serious drawback that causes failing drug therapy in disease control is non-compliance of patients that refuse the prescribed drugs by doctors for various reasons. By confirming all available problems and relatively weak effectiveness of other therapies, the third wave of psychological approaches are raised; which among third wave of therapies, acceptance and commitment-based therapy has a good ability to change internal and external verbal behaviors. It challenges references to commit the required changes in line with self-values and health. It uses acceptance and mindfulness strategies to increase cognitive flexibility. In terms of effectiveness, it is also applied as a relatively short-term and low-cost approach for a wide range of clinical conditions (12). From perspective of this therapeutic approach, pathology of hypertension is also the result of six processes: Avoiding experiences, cognitive fusion, lack of values, lack of presence in the present, dependence on the conceptualized self, and lack of commitment (13). In this therapeutic method, the patient is helped to examine his previous inefficient methods regarding his illness. It is attempted to show him how his methods have been ineffective to prevent and control his disease and may have exacerbated the problem. Then, he helps patients reduce their cognitive integration and connection as well as establishes better communication with their inner feelings. Finally, he identifies their personal values that have been disregarded so far, determines activities required to achieve these values, and commit to reach those (14). In the treatment approach, it is very important to create a cooperative relationship due to the fact that the relationship creates proper fields for treatment (15). In innovation of applying acceptance and commitment-based treatment to hypertension, we can refer the conducted works by Hayes et al. It is tried to show him how his methods have been ineffective to prevent and control his disease and may have exacerbated the problem. Then, he helps patients reduce their cognitive integration and connection as well as establish better communication with their inner feelings. Finally, he identifies their personal values that have been disregarded thus far, determines activities required to achieve these values, and commit to reach those (13). Therefore, no studies have been conducted to examine the effect of acceptance and commitment-based treatment to hypertension and variables of cognitive and excitement regulation simultaneously.
2. Objectives
Furthermore, by considering the chronic nature of hypertension, the present research was aimed to examine the effects of acceptance and commitment-based treatment to hypertension and cognitive excitement regulation among people with hypertension.
3. Methods
The present research is a pretest-posttest with control group that was conducted in a health center in the west of Ahvaz, Jundishapur University, in 2016 - 2017. Statistical population of the present study consists of all referred patients with hypertension to treatment clinics of Ahvaz who consume antihypertensive medications, however, they are still fluctuating hypertension. The present research sample includes 30 patients, by considering test power of 87%, significance level of 0.05, standard deviation of four, and by calculation 10% falling. The sampling was conducted during six months by primary interview to examine pharmacotherapy history and consuming drugs. It was conducted by using available sampling among all referred patients by considering the inclusion criteria. Finally, 30 patients agreed to participate in the research. They were classified in test and control groups (15 patients in each group).
In the present research, before intervention, blood pressure and score of cognitive regulation in both groups were identified. The inclusion criteria includes: (1) Patients with hypertension (hypertension than 140/90) who consume antihypertensive medications, however, they are still fluctuating hypertension; (2) have a diploma degree (due to various metaphors, intervention with acceptance and commitment-based treatment approach requires diagnosis power); (3) age ranges between 30 - 50 years old (patients with primary hypertension was the cause of selecting the range that in age more than 30 years old, their blood pressure will be increased and they will be sick due to reasons such as obesity, low movement, eating more salt, and other reasons); (4) lack of other clinic disorders simultaneously. The exclusion criteria include: (1) Unwillingness to continue to participate in the study and (2) absence of more than three out of 12 sessions.
Intervention contained 12, 90-minute session based on the acceptance and commitment treatment that was given only to the experimental group. In the last session, blood pressure and score of cognitive-emotional regulation for all subjects were evaluated (Table 1).
Table 1.
Research Plan Diagram
| Group | Random Assignment | Pre-Test | Intervention | Post-Test | Follow-Up |
|---|---|---|---|---|---|
| E | R | O1 | X | O2 | O3 |
| C | R | O4 | - | O5 | O6 |
3.1. Research Tools
3.1.1. Cognitive Emotion Regulation Questionnaire
Cognitive emotion regulation questionnaire (CERQ) is a self-evaluation questionnaire that has been designed and published by Garnefski et al. (12). Its structure is multi-dimensional and is used to identify cognitive coping strategies after a horrible experience. The cognitive excitement styles regulation questionnaire (CERQ) consists of 36 items. Each item is responded using the Likert five-point scale: (1) never; (2) sometimes; (3) generally; (4) often; (5) always. Then, the score of each nine-fold scale is calculated by considering the Table 2.
Table 2.
The Cognitive Excitement Styles Regulation Questionnaire Items
| Questions | |
|---|---|
| Positive cognitive regulation | 28, 26, 27, 25, 24, 23, 22, 21, 20, 19, 18, 17, 16, 15, 14, 13 |
| Negative cognitive regulation | 36, 35, 34, 33, 32, 31, 30, 29, 12, 11, 10, 9, 8, 7, 6, 5, 4, 3, 2, 1 |
| Compatible cognitive-emotional regulation factors | |
| Positive focusing/planning | 22, 21, 20, 19, 18, 17, 16, 14, 13 |
| Positive assessment/wider view | 27, 26, 25, 24, 23, 15 |
| Incompatible cognitive-emotional regulation factors | |
| Self-blame | 4, 2, 1 |
| Others’ blame | 36, 35, 34 |
| Rumination | 12, 11, 10, 9, 3 |
| Catastrophizing | 32, 31, 30, 29 |
| Acceptance | 8, 7, 6, 5 |
Mean while the questionnaire has no inverse questions.
This questionnaire can identify cognitive coping strategies and norm scores of different groups. The questionnaire is applicable in normal and clinical groups with the age of more than 12 years old. The questionnaire can assess cognitive styles of the public, especially those who had a negative experience. It can be applied in different age groups with different educational levels, mental patients, and normal individuals. Emotion regulation strategies in the questionnaire include positive and negative strategies as well as nine subscales. The subscales include five compatible subscales including acceptance (thinking with acceptance content and surrender to event), refocus (positive thinking to a pleasant and happy subject instead of thinking about the real event), refocusing planning (thinking about process of overcoming negative event or changing it), positive reappraisal (thinking about positive aspects of a private event or promotion), coming with view (thinking about low importance of an event or emphasis on its relativity in comparison with other events); and four incompatible subscales including self-blame (thinking with the content of guilt and blaming self), rumination (mental employment about emotions and thoughts related to negative events), catastrophizing (thinking with the content of horror of incident), and blaming others (thinking with the content of blame and blame others for what happened) (12). In the present research, 0.71 and 0.84 for Alpha Cronbach coefficients of cognitive excitement styles regulation questionnaire (CERQ) and cognitive regulations of incompatible excitement were calculated, respectively.
To assess the validity of the questionnaire in the Iranian population, it was first translated; then, in order to recognize psychometric properties and calculate validity along with 42 items of stress, anxiety and depression, it was applied for 250 adolescents aged 12 - 17 years old. Through correlation, a total score with scores of the subscales of the test, which its range was from 0.40 to 0.68 with average of 0.56 were examined. All of them were significant. In addition, there were respectively obtained coefficients of 0.35 and 0.37 for negative styles with depression scores and anxiety questionnaire with 28 general health questions that all of them were significant (13).
3.1.1.1. Blood Pressure Measuring Device
To measure blood pressure, after 15 minutes of rest in an upright position with the right arm twice within 30 seconds with a standard mercury sphygmomanometer Japanese Alp K2 armband arm circumference, depending on size of the wind and mercury in systolic and diastolic blood pressure column contained two degrees. A general practitioner measures and records blood pressure; the average of the two measurements will be taken into account. Hypertension has been defined according to criteria of 7th report of the National Committee for Prevention, Detection, and Treatment of High Blood Pressure as a systolic blood pressure higher than 140 mmHg or a diastolic pressure more than 90 mmHg.
3.1.1.2. Educational and Treatment Program
In the present research, we used acceptance and commitment therapy as treatment approach. In this therapeutic approach, instead of changing cognitions, it is tried to increase individual’s psychological relationship with his thoughts and feelings about his disease. In the present study, this therapeutic intervention was used by considering treatment protocol of Vowel and Sorel (16). According to the Table 3, an educated person who has a valid certificate in this area presented interventions to the experimental group.
Table 3.
A Summary of Acceptance and Commitment Therapy Protocol
| Meetings | Content | Target |
|---|---|---|
| First session | The questionnaire completion, blood pressure measurement, familiarity with group and its rules, familiarity with proper treatment and conceptualization assessment. | The questionnaire completion, conceptualization assessment |
| The second session | Reviewing homework and examining behavior or situations of sculptor, its causes and consequences, creative disappointment; in other words, reducing tendency to control thoughts and feelings through metaphor. | Discussing experiences and evaluating them, creating creative desperation |
| Third session | Introducing control as a problem (discussing control of thoughts and feelings) and introducing tendency using metaphor. | Control as a problem and introducing tendency |
| Fourth Session | Introducing fault through metaphor, introducing clean and foul suffering, and reducing dependence on hypertensive disabling thoughts. | Introducing fault |
| Fifth session | Introducing self as a field through metaphor and discussion about reducing personal interest in individual events. | Introducing self as a field |
| Sixth session | Using mindfulness techniques and emphasize on being the present time through metaphor. | Mindfulness Practice |
| Seventh session | Specifying values by answering the question: What you want to look for in your life, and discussing prioritizing values. | Setting values |
| Eighth session | Understanding nature of willingness and commitment, engaging in action using metaphor. | Commitment behavior |
| From 9th to 12th sessions | Reviewing the sixth and seventh sessions, completing the questionnaire and measuring blood pressure. | Increasing the effectiveness of treatment and completing the questionnaire |
Data were analyzed using SPSS-21 software and using covariance multi-variable analysis (MANCOVA). The significance level was considered less than 0.05. The ethical considerations were considered in accordance with the Helsinki Law. The study objectives were explained for the patients and were provided an opportunity to ask questions. Patients were also assured that their complications would not be threatened by them, that they did not interact with their treatment process, and that they could opt out of cooperation at any time. Consent from all patients was received and it was also assured that their information was confidential and only used in this study.
4. Results
According to the research findings in Table 4, mean age of experimental group was 43.29 ± 5.08 and mean age of the control group was 42.18 ± 5.12. Number of males in the experimental and control groups was 13 (60%) and 10 (63.66%) respectively; the number of the employed patients in the experimental and control groups was 11 (73.33%) and 10 (63.66%) respectively; meanwhile, 13 (86.66%) and 14 (93.33%) patients in experimental and control groups were married, respectively; of course, 100% of subjects in both groups were under medical treatment.
Table 4.
Demographic Characteristics of Test and Control Groupsa
| Variable | Test Group | Control Group | P |
|---|---|---|---|
| Age | 43.29 ± 5.08 | 42.18 ± 5.12 | 0.547 |
| Gender (male) | 13 (86.66) | 10 (63.66) | 0.456 |
| Employment (employed) | 11 (73.33) | 10 (63.66) | 0.214 |
| Married status | 13 (86.66) | 14 (93.33) | 0.138 |
| Under medical treatment | 15 (100) | 15 (100) | 0.315 |
aValues are expressed as No. (%).
Table 5 showed that in the experiment group, average scores of adaptation cognitive regulation in pre-test and post-test were 26.47 and 13.56 respectively. In addition, in the control group, average scores of adaptation cognitive regulation in pre-test and post-test are 40.59 and 13.56, respectively.
Table 5.
The Mean and Standard Deviation of the Highest and the Lowest Score of Cognitive Emotional Regulation in the Experimental and Control Groups in Pre-Test and Post-Test
| Step/Statistical Indices of Groups | Mean ± SD | The Most | The Least |
|---|---|---|---|
| Pre-test | |||
| Experiment | 26.47 ± 7.76 | 63 | 40 |
| Control | 13.56 ± 16.73 | 75 | 35 |
| Post-test | |||
| Experiment | 40.59 ± 6.17 | 70 | 48 |
| Control | 13.56 ± 17.22 | 79 | 40 |
Table 6 showed that in the experiment group, average scores of incompatible cognitive regulation in pre-test and post-test were 46.51 and 47.66, respectively. In addition, in the control group, average scores of incompatible cognitive regulation in pre-test and post-test were 41.93, 47.60 respectively.
Table 6.
The Mean and Standard Deviation of the Highest and the Lowest Score of Incompatible Cognitive Emotion Regulation in the Experimental and Control Groups in Pre-Test and Post-Test
| Step/Statistical Indices of Groups | Mean ± SD | The Most | The Least |
|---|---|---|---|
| Pre-test | |||
| Experiment | 46.51 ± 3.96 | 58 | 46 |
| Control | 47.66 ± 16.73 | 96 | 30 |
| Post-test | |||
| Experiment | 41.93 ± 5.41 | 53 | 34 |
| Control | 47.60 ± 21.26 | 30 | 97 |
As seen in Table 7, there is a significant difference between the two groups (P < 0.05 and F = 18.51). Therefore, the first hypothesis of this study is confirmed. This result means that educating acceptance and commitment-based treatment has been effective for the hypertension of subjects in the experimental group in post-test, as well as decreased hypertension.
Table 7.
Summary Results of the ANOVA Analysis to Compare Mean of Pre-Test and Post-Test in Hypertension by Controlling Pre-tests in Experimental and Control Groups
| Source of Change | Sum of Squares | DF | Average of Squares | F | P Value | ETA Coefficient | Statistical Power |
|---|---|---|---|---|---|---|---|
| Pre-test | 1.450 | 1 | 2.450 | 4.71 | 0.04 | 0.18 | 0.27 |
| Group | 26.241 | 1 | 26.241 | 18.51 | 0.0001 | 0.40 | 0.99 |
| Error | 38.03 | 27 | 1.40 | ||||
| Total | 21.4107 | 30 |
Table 8 showed a significant difference between experimental and control groups, in terms of dependent variables at P < 0.05. Therefore, at least in one of the dependent variables (compatibility and incompatibility cognitive emotion regulation), there is no significant difference between the two groups. Effectiveness is 0.71 in the study.
Table 8.
Results of Multivariate Covariance Analysis on the Mean Score of Post-Test Cognitive Emotion Regulation (Compatibility and Incompatibility) in the Experimental and Control Groups
| Test Name | Level | F | Error DF | Hypothesis DF | Effect | P Value |
|---|---|---|---|---|---|---|
| Piley effect test | 0.71 | 31.65 | 25 | 2 | 0.71 | 0.001 |
| Lambda’s wikis test | 0.28 | 31.65 | 25 | 2 | 0.71 | 0.001 |
| Hotelling effect test | 2.53 | 31.65 | 25 | 2 | 0.71 | 0.001 |
| The biggest root test | 2.53 | 31.65 | 25 | 2 | 0.71 | 0.001 |
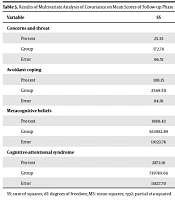
According to Table 9, it can be seen that there is a significant difference between experimental and control groups in post-test, in terms of variable of cognitive emotion regulation at P < 0.05. In addition, the effect coefficient shows that 37% of difference between the two groups in the post-test is related to experimental intervention, in terms of cognitive-behavioral adjustment.
Table 9.
Results of ANCOVA Analysis in Context of MANCOVA on Average Post-Test Score of Cognitive Emotion Regulation (Compatibility and Incompatibility) in Experimental and Control Groups
| Test Name | Sum of Squares | DF | Average of Squares | F | Effect | P Value |
|---|---|---|---|---|---|---|
| Compatibility cognitive emotion regulation | 276.72 | 1 | 276.72 | 15.69 | 0.37 | 0.001 |
| Incompatibility cognitive emotion regulation | 448.21 | 1 | 448.21 | 33.77 | 0.56 | 0.001 |
5. Discussion
This study aimed to evaluate the effectiveness of acceptance and commitment-based treatment to hypertension and cognitive emotion regulation in hypertensive patients in Ahvaz. The research results showed that acceptance and commitment-based treatment affects decreasing hypertension in patients with high blood pressure. The research results were consistent with the obtained results by Hayes et al. (13) and Hayes (14).
Hypertension is one of the most common, chronic, and relapsing diseases among patients that can cause other diseases, while it can be prevented in the present age. Due to extensive and long-term changes in behavior related to lifestyle, it is a difficult and challenging disorder in therapeutic viewpoint. On the other hand, the more people who control their emotions and dominate life, especially in more stressful situations, have a greater sense of inner satisfaction of their lives, which is important for their health. Acceptance and commitment-based treatment helps people identify situations that make their blood pressure rise by metaphor, and can train ways to deal with those situations during the treatment process. In acceptance and commitment-based treatment, a therapist efforts identifying values of the patient and cultivating a life based on his value, which according to the values, he helped authorities find the best way to live and commit themselves to it (17). In regards to acceptance and commitment-based treatment to hypertension, Harris (18) believes that transparency of values during the treatment will encourage group members to be motivated to continue treatment and commitment acts when values are clear. In addition to these two important processes of acceptance and commitment-based treatment, namely connection with the present time and self as the field, they cause increasing their knowledge regarding regular continuous hypertension check, exercise, and healthy eating.
In addition, the research results showed that acceptance and commitment-based treatment is confirmed by increasing compatibility cognitive emotion regulation among people with hypertension. The research findings are consistent with the obtained results by Gorgui et al. (19), Christensen et al. (20), and Todarello et al. (21). Due to the fact that emotions are socially useful and they can be effective to transfer emotions to others, social interaction, and create and maintain constructive relationships with others, their adjustments can play an effective role on mental health and its related variables. By improving excitement regulation, automatic state of behavioral reactions will be slow and will manage his behaviors, rather than act in a pulse state. In addition, calm and relaxation in this intervention to stabilize the nervous system and emotional control all lead to positive cognitive emotion regulation strategies. Acceptance and commitment therapy believes that a particular form of knowledge leads to recognition, and changing quality of level of awareness can save a person from thinking. According this treatment method, most people are involved in their internal experiences and it seems that the situation is a result of reality. Thus, instead of just experiencing anger, we are angry, we can hate rage, and we wish anger away from us. On the contrary, such answers involve us in their excitements and we try to avoid them (17). Therefore, by changing the quality of people’s knowledge, it can be seen that their use from cognitive strategies to regulate emotion will be increased. Acceptance and commitment therapy may act in two ways: (a) It will encourage people to view their mental processes, see and accept self-critical and judgmental thoughts, and try to focus on them and (b) emphasis on self-acceptance may lead to re-evaluate thoughts of a person. Hayes et al. also believes that acceptance and commitment therapy approach helps referees accept their emotional and cognitive control and get rid of controlling thoughts that caused their problems rather than focusing on elimination of the damage-causing factors (13).
5.1. Conclusions
The research findings suggest that acceptance and commitment-based treatment approach can be effective as a non-pharmacological, easy, and safe complementary therapy in improving the state of hypertension in people with hypertension who are also treated by drugs but still have high blood pressure. Therefore, health policy makers should pay particular attention to this complementary methodology and they should plan further research in this field and use this method in the clinical field to improve conditions of these patients, which is the main goal of the treatment. Knowledge of custodians, especially physicians, psychologists, and nurses, should be increased and encouraged to use this method in conjunction with routine care.
The research limitations included: (1) its sample included individuals with hypertension who were also associated with hypertension due to drug use. Therefore, we should consider caution matters to generalize the research results to other groups of society and other diseases; (2) due to criterion-centric sampling method, many samples had no entry criteria or were excluded from the study due to exclusion criteria; therefore, a large volume of patients with hypertension, especially illiterate or aged people, did not get psychotherapy.