




1. Background
Head and neck cancer is one of the most prevalent malignancies around the world (1). This malignancy most commonly includes the neoplasms of the oral cavity, followed by skin, lips, nasal cavity and paranasal sinuses, salivary glands, pharynx, and larynx (2). South Asian areas including Pakistan are recognized as high-risk geographical regions for this type of cancer (3) while it is found rarely in developed countries such as the UK (4).
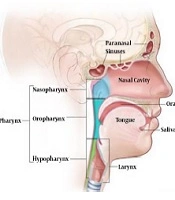
Head and neck cancer is a broad term that includes various types of cancer (tumors) in the upper aerodigestive tract, including the lip, mouth, nose, tongue, throat, oral cavities, sinuses, pharynx, and vocal cords (larynx), as well as some other sites in this anatomical part as shown in Figure 1 (5). Squamous cell carcinomas account for about 90% of these cancers, which are the most frequently observed malignancies of the head and neck site, occurring possibly due to the excessive use of alcohol and tobacco (6). Head and neck cancer ranks sixth among all cancers in the world with about 630,000 new patients registered per year leading to 350,000 deaths annually. The five-year survival rate of patients with head and neck squamous cell carcinoma is around 45% - 55% (7).

Anatomy of head and neck cancer
It has been observed that the chance of developing head and neck cancer is relatively higher in Pakistan, particularly Karachi (the urban area of Sindh), than any other region in the world. It is due to the habitual involvement of a large number of people in smoking and chewing Chalia and Gutka. The incidence rate of head and neck cancer has been noted as 10 per 100,000 population in countries such as Pakistan, India, and Sri Lanka. The five-year survival rate of head and neck cancer is below 40% (8). The largest city of Pakistan, Karachi, ranks highest in the globe with regard to the incidence of oral cavity cancers (9). In recent years, the rural areas of Sindh have been the victims of growing malignancies of head and neck but accurate statistics and data have not been published to indicate the factual position of rural areas.
The frequent use of betel nut, betel quid, and pan masala enhances the probability of developing head and neck cancer (10). Studies in Pakistan show that betel, areca, and tobacco chewing may lead to 8.5 to 10 times increased risk of oral cancers, after adjusting for covariates (11). According to research, 58% of the total head and neck cancers in the world occur in the south and southeast Asia owing to the persistent use of chewing tobacco (12).
Both males and females in Pakistan are prone to the malignancies of head and neck but males are more affected as they, with the rates of 66% to 95%, are the main victims of this fatal disease (13). The ratio of pharyngeal and oral cavity cancers among males and females is around 3 to 1 (14). The incidence of head and neck cancer is estimated to be higher in older people than in younger ones (12).
Nuclear Medicine Oncology and Radiotherapy Institute Nawabshah (NORIN) is among a few tertiary healthcare facilities in the rural areas of Sindh, Pakistan, which specifically operates for diagnosis, treatment, and research of different types of cancer. NORIN started its clinical oncology and radiotherapy services in January 2012.
2. Objectives
The goal of the present study was to find the factual position of head and neck cancer in rural areas of Sindh. Although the obtained data are not based on a detailed survey, in the absence of any detailed national level population-based cancer database, they can be considered a reliable source of information regarding the occurrence and frequency of different types of head and neck cancer in rural areas of Sindh. NORIN is a tertiary cancer care center whose statistical data might differ from other cancer hospitals situated in other areas of Pakistan (15).
3. Methods
The present study was conducted at Nuclear Medicine Oncology and Radiotherapy Institute Nawabshah (NORIN), Sindh, with the aim of reviewing descriptive epidemiological characteristics and incidence of head and neck cancer from January 2012 to December 2016. All the data were collected from manual records, which were gathered during this period and verified from hospital data base system. In this study, we divided head and neck cancer patients according to their gender, age, districts, tumor location, and stage of cancer when they were admitted to the Clinical Oncology and Radiotherapy Department of NORIN. The diagnosis and staging were based on international protocols and International Classification of Disease-oncology by experienced oncologists.
4. Results
In total, 3,400 patients were registered at the Clinical Oncology Department of NORIN for all malignancies in five years, 31% of whom were head and neck patients. Among 1,030 patients with head and neck cancer, 56% were male patients and 44% were female patients, as shown in Figure 2. The data were sub-categorized according to the site of tumor, which showed 596 (58%) of head and neck cancer patients were affected by oral cavity, followed by tongue (21%), tonsil (4%), floor of the mouth (10%), gum (5%), hard palate (9%), soft palate (3%), and lips (5%). Moreover, 22.1% of head and neck cancers were in the hypopharynx, 5% in the nasopharynx, 5% in oral-pharynx, 4% in larynx, 3% in the parotid gland, and 3% in the salivary gland, as shown in Figure 3.

Gender wise distribution of head and neck cancer patients at NORIN

Distribution of cancer patients respecting malignancies
Figure 4 compares the number of head and neck cancer patients registered at NORIN during the last five years according to the stage of the disease. We observed that 2.2% of the total head and neck cancer patients were diagnosed at stage I, 7.9% at stage II, 37.7% at stage III, and 45.6% at stage IV. Moreover, 6.6% of the patients were observed to have metastases of unknown origin, as shown in Figure 5. All head and neck cancer patients are curable if diagnosed at early stages. Unfortunately, 83% of the patients reported during 2012 - 2016 were at stage III or IV of disease, with malignancies spreading to a distant site at the time of diagnosis. It is reported that the majority of head and neck cancer patients in Pakistan are diagnosed at stage III and stage IV (14). The probable causative agents for head and neck cancer observed at NORIN in this study are shown in Figure 6.

Number of head and neck cancer patients in the last five years

Number of head and neck cancer patients diagnosed at different stages

Probable causative agents for head and neck cancers at NORIN
Age-wise distribution of patients is shown in Figure 7. Overall, 75% of all head and neck cancer patients were 40 - 85 years of age (26% aged 40 - 50 years, 23% aged 50 - 60 years, and 27% aged 60 - 85 years), 23% were 20 - 40 years of age (7% aged 20 - 30 and 15% aged 30 - 40 years), and 2% were in the children group. Patients from all over the country, particularly rural areas of Sindh, were registered at NORIN. District-wise data are shown in Figure 8. The majority of patients belonged to Nawabshah and its neighboring areas.

Age-wise distribution of head and neck cancer patients in the last five years at NORIN

Districts of the rural areas of Sindh, Pakistan
5. Discussion
Here we presented head and neck cancer data from one comprehensive tertiary care cancer hospital. The results showed that patients suffering from head and neck cancer were aged between 40 and 85 with male predominance. Major reasons for head and neck cancer in these patients are the lack of awareness, education, and diagnostic facilities. The data showed that most patients started cancer treatment at the third and fourth stages of disease, which makes it very difficult to cure. Smoking and the use of alcohol, Gutka, Supari, Naswar, Man-Pori, etc., are the main causes of head and neck cancer in rural areas.
It is possible that the number and percentage of different head and neck cancers vary in this area from other areas. A study (16) showed that the extensive use of Betelnut, Pan, Gutka, and tobacco in the forms of smoking (cigarette, Biddi) or chewing (Naswar, Nass) may raise the risk of cancer of head and neck, especially in the oral cavity. A study (17) showed age-specific cancer incidence in urban areas but such data are not available for rural areas of Pakistan. Some radiotherapy centers situated in urban areas of Pakistan such as KIRAN cancer hospital, Karachi Jinnah hospital, Lahore AFIP Hospital, and Rawalpindi conducted retrospective analysis of head and neck cancer data (15) but no similar study was found at radiotherapy centers situated in rural areas of Sindh.
5.1. Conclusions
Head and neck malignancies are the most common type of cancer registered at NORIN in the last five years. Because of the lack of awareness, education and diagnostic facilities, most patients start cancer treatment at the third and fourth stages of disease, which makes it very difficult to cure. It is concluded that patients suffering from head and neck cancer have an age between 40 and 85 with male predominance. Smoking and the use of alcohol, Gutka, Supari, Naswar, Man-Pori, etc., are the main causes of head and neck cancer in rural areas. Central cancer databases, media awareness campaigns for general populations, and informative lectures in educational institutes may be undertaken to prevent head and neck cancer. In addition, screening programs, pictorial hazards of chewing tobacco and betel, the complete government ban on the use of Gutka, Supari, and Manipuri, and introduction of new diagnostic facilities for early detection are necessary to efficiently fight head and neck cancer. More studies are suggested to indicate the factual position of rural areas of Pakistan.
