



1. Background
Diabetes Mellitus (DM) is a chronic metabolic disorder caused by impaired insulin release, insulin function, or both, which includes 90% of all types of diabetes (1, 2). Diabetes Mellitus has a growing trend in recent years and was increasingly prevalent. According to the World Health Organization (WHO), adults with DM throughout the world were 422 million in 2014, which is expected to reach over 366 million by 2030 (3). In Iran, it is estimated that the number of people with diabetes will reach 9.2 million by the year 2030 (4).
Various factors have been identified as risk factors of DM, including smoking, being overweight and obese, low physical activity, hypertension, high cholesterol, and genetic (5, 6). Moreover, DM has many chronic complications, including decreased physical function, mental health problems, impaired personal and interpersonal relationships, neuropathy, nephropathy, retinopathy, and cardiovascular disorders (7, 8). Also, high levels of low-density lipoprotein (LDL) and very-low-density lipoprotein (VLDL), and low levels of high-density lipoprotein (HDL) with high blood pressure in patients with DM make them more susceptible to atherosclerosis, which is the most common cause of death in these patients type II DM (8).
Exercise is one of the therapeutic options for patients with DM, which lowers blood glucose, glycosylated hemoglobin, and cardiovascular risk factors, and prevents long-term complications of DM. Walking is one of the activities that has a positive effect on diabetes and leads to increased norepinephrine, serotonin synthesis, and endorphins, which are effective in causing vitality and preventing fatigue in people with diabetes (9, 10). Walking is a simple sport that does not require any special equipment and can be combined in the daily life of people with DM (11, 12). In this regard, the study by Yekkeh Fallah et al. showed that walking is effective in lowering blood sugar in patients with DM (13).
Yoga is another exercise that enhances muscle flexibility and strength, and also improves blood circulation, oxygen uptake, and hormone function. In addition, yoga stabilizes the autonomic nervous system, controls emotions, and improves one's sense of health (13, 14). Various studies have investigated the effects of yoga that have reported different results (13, 15, 16). For example, the study of Yekkeh Fallah et al. showed that decrease in fasting blood sugar (FBS) at the end of the intervention in the yoga group was significant (13), but Sreedevi et al. (15) and Shiju et al. (16) did not report significant changes in FBS and lipid profile.
Although the effects of walking and yoga on improving some laboratory and clinical indicators have been identified separately, there is no enough knowledge about the effectiveness of these two methods compared to each other. Therefore, it is necessary to compare these two activities so that we can recommend the most appropriate method to patients. Therefore, this study aimed to compare the effect of walking and yoga on the clinical and laboratory parameters in men with type II DM.
2. Objectives
The aim of this study was to compare the effect of walking and yoga on clinical and laboratory indicators in men with type II DM.
3. Methods
This randomized clinical trial (IRCT20180511039610N1) was conducted with a pre-test/post-test design on 108 men with type II DM referring to Golestan and Imam Khomeini and hospitals in Ahvaz, Iran, from May to August 2019. The sample size was calculated as 108 individuals using table B.12 (17) and considering 10% attrition and α = 0.05, β = 0.95, and Δ/σ ~ 1 according to the previous studies (9).
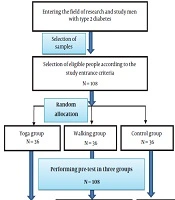
The inclusion criteria were men aged 30 to 65 years, at least 1 year has been passed since the diagnosis of DM, not participating in another exercise programs at the same time, lack of exercise prohibitions, lack of any physical activity limitations, lack of insulin treatment, and not taking antidepressants. The exclusion criteria were hospitalization during the intervention, change of treatment from oral medications to insulin therapy during the study period, migration to another city, and medical forbiddance for physical activity during the intervention. One hundred and eight eligible men were randomly assigned to walking (n = 36), yoga (n = 36), and control (n = 36) groups using a block permutation method with block size 6. The random allocation was made by a statistical consultant who was a member of the research team (Figure 1).

CONSORT flowchart
After the random allocation of the patients to the groups, the pre-test was conducted in all three groups. The walking group was asked to walk for 8 weeks three times a week for 60 minutes each time. The yoga group also received yoga training for 8 weeks, 3 sessions a week, and 60 minutes each time, under the supervision of the researcher and professional instructor in a designated gym. Yoga included warm-up, physical and breathing exercises, relaxation, and meditation. The control group did not receive any intervention. A post-test was conducted on the three groups at the end of the eighth week of interventions.Data collection tools were a demographic information questionnaire (containing questions about age, occupation, educational level of the patient and his wife, economic status, history of hospitalization), mercury sphygmomanometer (Yamaso Model 600), and height and weight scale (Seka model 786). The same tools were used for all participants, and the tools were calibrated before use. Simultaneous measurements of height, weight, and blood pressure were performed by two people, including the researcher and a research assistant nurse. To perform biochemical tests, a blood sample of 10 ml was taken in two stages (pre-test and post-test) in the fasting state by the researcher. All blood samples were evaluated using quantitative diagnostic kits (fasting blood sugar: FBS, Cholesterol, Triglycerides: TG, HDL-C, and LDL-C) of Pars Azmun Company after storage at -70°C. All participants' blood tests were evaluated in the same laboratory.
Data analysis was performed using SPSS software version 20. To examine the relationship between qualitative variables, the chi-square test was used and to compare quantitative variables between three independent groups (yoga, walking, and control), one-way analysis of variance, or its non-parametric equivalent (Kruskal-Wallis test) was used. The Mann-Whitney test was used to determine the mean difference between the independent groups, and the Wilcoxon test was used to compare the mean within the groups. The significance level was considered to be less than 0.05.
3.1. Ethical Considerations
This study was approved by the Research Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (IR.AJUMS.REC.1397.101). Ethical considerations included explaining essential information to participants, obtaining informed consent, voluntary participation in the study, freedom in leaving the study at any time, the confidentiality of the information, and no imposing costs on the participants.
4. Results
In this study 108 men with type II DM participated. Their mean (standard deviation: SD) age was 49.91 (9.42) years. The mean (SD) of participants’ height was 170.99 (7.02) cm, weight was 81.82 (9.73) kg, Body Mass Index (BMI) was 28.06 (3.31) kg/m2, and systolic blood pressure (SBP) and diastolic blood pressure (DBP) were 135.22 (13.71) and 83.48 (8.80) mmHg, respectively. There was no statistically significant difference between the three groups in terms of demographic characteristics (Table 1).
| Variables | Groups | P Value | ||
|---|---|---|---|---|
| Yoga | Walking | Control | ||
| Occupationb | 0.126 | |||
| Employee in governmental sections | 2 (5.6) | 5 (13.9) | 6 (16.7) | |
| Self-employed | 24 (66.7) | 16 (44.4) | 23 (63.9) | |
| Unemployed | 5 (13.9) | 3 (8.3) | 3 (8.3) | |
| Other | 5 (13.9) | 12 (33.3) | 4 (11.1) | |
| Educationb | 0.518 | |||
| Illiterate | 1 (2.8) | 3 (8.3) | 1 (2.8) | |
| Primary school | 15 (41.7) | 11 (30.6) | 11 (30.6) | |
| High school diploma or associate degree | 18 (50) | 17 (47.2) | 22 (61.1) | |
| Bachelor’s degree and above | 2 (5.6) | 5 (13.9) | 2 (5.6) | |
| Financial statusb | 0.249 | |||
| Good | 2 (5.6) | 4 (11.1) | 4 (11.1) | |
| Average | 29 (80.6) | 20 (55.6) | 23 (63.9) | |
| Weak | 5 (13.9) | 12 (33.3) | 9 (25) | |
| History of hospitalizationb | 0.510 | |||
| Yes | 12 (33.3) | 15 (41.7) | 11 (30.6) | |
| No | 24 (66.7) | 21 (58.3) | 25 (69.4) | |
| Education of spouseb | 0.634 | |||
| Illiterate | 3 (8.3) | 4 (11.1) | 5 (13.9) | |
| Primary school | 14 (38.9) | 21 (58.3) | 16 (44.4) | |
| High school diploma or associate degree | 18 (50) | 10 (27.8) | 14 (38.9) | |
| Bachelor’s degree and above | 1 (2.8) | 1 (2.8) | 1 (2.8) | |
| Agec | 48.25 ± 7.14 | 49.83 ± 9.58 | 51.66 ± 11.06 | 0.308 |
aValues are expressed as No. (%) or mean ± SD.
bChi-square test.
cOne-way ANOVA.
The results showed that there was no difference between the mean scores of the clinical and laboratory parameters between the three groups before the intervention (P > 0.05). However, data analysis of post-test showed significant differences in the mean scores of FBS (P = 0.045), LDL (P = 0.005), HDL (P = 0.001), SBP (P = 0.002), DBP (P = 0.003), and BMI (P = 0.024) between the three groups after the intervention. There were no significant differences between the three groups in terms of TG (P = 0.163) and cholesterol levels (P = 0.061) (Table 2).
| Variables | Before Intervention | After Intervention | P Valueb |
|---|---|---|---|
| FBS (mg/dL) | |||
| Yoga | 181.11 (56.48) | 159.62 (49.40) | < 0.0001 |
| Walking | 162.66 (59.89) | 165.30 (64.81) | 0.668 |
| Control | 179.05 (75.03) | 195.57 (63.37) | 0.022 |
| P valuec | 0.232 | 0.045 | |
| LDL (mg/dL) | |||
| Yoga | 80.97 (30.07) | 79.34 (25.83) | 0.724 |
| Walking | 84.67 (35.79) | 83.24 (29.10) | 0.872 |
| Control | 88.91 (28.66) | 101.81 (29.17) | 0.001 |
| P valuec | 0.478 | 0.005 | |
| HDL (mg/dL) | |||
| Yoga | 46.25 (9.02) | 48.71 (7.53) | 0.107 |
| Walking | 45.52 (11.16) | 48.49 (10.91) | 0.022 |
| Control | 42.30 (7.72) | 41.96 (7.07) | 0.274 |
| P valuec | 0.150 | 0.001 | |
| TG (mg/dL) | |||
| Yoga | 151.02 (87.07) | 139.68 (71.81) | 0.166 |
| Walking | 161.11 (93.75) | 149.45 (99.06) | 0.245 |
| Control | 161.11 (91.64) | 171.21 (82.63) | 0.391 |
| P valuec | 0.809 | 0.163 | |
| Cholesterol (mg/dL) | |||
| Yoga | 154.61 (42.04) | 145.65 (38.37) | 0.003 |
| Walking | 151.40 (42.14) | 149.09 (35.28) | 0.681 |
| Control | 163.52 (31.31) | 166.15 (36.12) | 0.754 |
| P valuec | 0.426 | 0.061 | |
| SBP (mmHg) | |||
| Yoga | 134.44 (13.61) | 127.34 (11.07) | 0.001 |
| Walking | 132.05 (13.53) | 126.36 (11.94) | < 0.0001 |
| Control | 139.16 (13.38) | 136.66 (12.16) | 0.059 |
| P valuec | 0.062 | 0.002 | |
| DBP (mmHg) | |||
| Yoga | 82.08 (8.81) | 82.03 (6.93) | 0.824 |
| Walking | 82.38 (9.54) | 81.66 (7.03) | 0.514 |
| Control | 85.97 (7.63) | 86.51 (5.22) | 0.533 |
| P valuec | 0.222 | 0.003 | |
| BMI (kg/m2) | |||
| Yoga | 28.45 (3.06) | 27.88 (2.77) | 0.001 |
| Walking | 27.01 (2.92) | 26.69 (3.03) | 0.07 |
| Control | 28.72 (3.74) | 28.82 (3.68) | 0.761 |
| P valuec | 0.058 | 0.024 |
Abbreviations: BMI, body mass index; DBP, diastolic blood pressure; SBP, systolic blood pressure; TG, triglycerides.
aStatistically significant (P < 0.05).
bWilcoxon test.
cMann-Whitney U test.
The comparison of groups using Post hoc test showed that there were statistically significant differences after intervention between the two groups of walking and control in terms of FBS level (P = 0.028); between the two groups of yoga and control (P = 0.007) and walking and control groups (P = 0.033) in terms of LDL level; between the two groups of yoga and control (P = 0.001), and the two groups of walking and control (P = 0.016) in terms of HDL level. Moreover, significant differences were seen between the two groups of yoga and control (P = 0.004) and the two groups of walking and control (P = 0.001) in SBP; and between yoga and control (P = 0.02) and walking and control (P = 0.005) groups in DBP. Regarding BMI, there was a significant difference between the two groups of walking and control (P = 0.027).
5. Discussion
In this study that was carried out with the aim of comparing the effects of walking and yoga on the clinical and laboratory parameters in men with type II DM, the findings revealed that walking and yoga training had an effective role in improving clinical and laboratory parameters in men with type II DM.
Accordingly, the results indicated that there was a significant difference in mean of FBS, LDL, HDL, SBP, and DBP, and BMI indices between the three groups of yoga, walking, and control after the intervention, but cholesterol and TG levels showed no significant differences in the three groups. The yoga group showed a greater decrease in FBS, cholesterol, and BMI compared to the walking group. However, the decrease in SBP was more in the walking group than that in the yoga group. The inter-group comparisons showed a statistically significant difference in the mean of BMI in the two groups of walking and yoga, which was in favor of the yoga group, but there was no significant difference between the two groups in other indices. Consistent with the present study, the study by Sreedevi et al., which aimed to determine the effect of yoga and peer support on blood sugar (BS) in women with type II DM, showed that the mean of SBP decreased significantly after yoga intervention (15). However, the results of Kim et al. did not show such effectiveness (18). The difference between the results of the researches can be attributed to the difference between the intensity and duration of the training programs as well as the difference between the age and gender of the research samples. In a study by Rafiei et al., with the purpose of comparing the effect of Tai Chi exercise and walking on FBS in patients with type II DM, there was a significant difference between the mean of BS levels before and after the intervention in the Tai Chi and walking groups. Although FBS in the walking group had more decline than in Tai Chi and control groups, the difference was not significant (19). Yekkeh Fallah et al. in their study which aimed to compare the effect of one month of regular yoga and walking exercises on BS and the number of pills used in type II DM patients, declared that there was a significant decrease in FBS at the end of the intervention in the yoga group, but it was not significant in the walking group (13). In a study by Bello-Ovosi et al., who aimed to investigate the effects of aerobic exercise on physiological parameters and quality of life in patients with type II DM, the results showed that FBS, LDL, and HDL were significantly improved significantly in the intervention group (20). Chimkode et al., in a study with the purpose of investigating the effect of yoga on blood glucose levels in healthy and diabetic subjects, reported that yoga practices led to a significant reduction in the mean of fasting and after-breakfast BS levels in the diabetic group compared to the healthy group (2). However, some studies have shown no significant changes in clinical and laboratory parameters of patients after exercise interventions (15, 16). For example, in the study by Sreedevi, cholesterol level, FBS, and BMI did not change significantly after the intervention (15). Also, the results of a study by Shiju et al. showed that yoga intervention did not change or improve the BS level and lipid profile of studied patients (16). In the study by Dabbagh Nikukheslat et al. (21), BMI did not show any significant change after the intervention. Shantakumari et al. reported that after performing yoga exercises, although BMI decreased and HDL levels increased in type 2 DM patients, it was not statistically significant. They stated that yoga exercises significantly reduced cholesterol, TG, and LDL levels in the intervention group (22). It seems that practicing yoga exercises and regular walking in proper time intervals can improve some of the laboratory and clinical parameters. Based on the results of various studies as well as the present study, what is understood is that it is not possible to say with certainty which of the two methods of walking and yoga is superior to the other. So patients can take advantage of any of these exercises that they find more enjoyable.
One of the limitations of this study, which limited decision-making to more effective intervention, was the failure to measure glycosylated hemoglobin (HgA1C) due to time constraints. Another limitation of the present study was that it was not possible to observe the exact course of walking and its severity in patients in the walking group, so the self-report method was used to evaluate it, and patients were monitored by telephone. Therefore, further studies are recommended with careful control of activity intensity, as well as by measuring HgA1C to determine the effectiveness of the intervention in controlling BS over time.
5.1. Conclusions
The findings of the study show that yoga and walking exercises improve the FBS level and lipid profile, especially cholesterol and HDL levels in men with type II DM. Yoga and walking exercises are also effective in reducing SBP and BMI. However, in comparison to walking, yoga had a more desirable effect on lowering the levels of FBS and cholesterol in the patients. Therefore, considering the effectiveness of yoga and walking exercises, it is recommended to consider these exercises in the training and self-care programs of patients with diabetes. It is likely that the duration of training in these patients should be longer for further influence on other parameters (TG and LDL).
