


1. Background
Breast cancer (BC) is one of the most common cancers in women (1). Its global prevalence increased by 3.1% from 1980 to 2010. In addition, it has claimed 521,817 lives, according to the reports, in 2012 (2, 3). According to the statistics of the profile of Iran's cancer indicators announced to the World Health Organization (WHO), in 2014, 9795 Iranian women were diagnosed with BC, causing an annual death rate of more than 10 per 100,000 women (4, 5). In its early stage when the tumor is small, BC has no symptoms. However, as the tumor grows, one or more symptoms and signs may appear, including a painless lump in the breast, a lump under the armpit, breast pain, swelling or thickness of the breast skin, spontaneous discharge of the nipple particularly blood, and erosion or inversion in the nipple (6).
Knowledge of these symptoms and risk factors of BC, as well as having a positive attitude to screening and early diagnosis of the disease, play a significant role in the performance and preventing the disease while decreasing the mortality rate (6-9). Although merely having a high level of knowledge may not lead to appropriate performance for breast self-examination, clinical breast examination, and mammography, studies have shown that higher mortality rates of cancers are related to lack of knowledge and late-stage diagnosis (10, 11). In addition, a study indicated that identifying individual and clinical factors related to BC can provide basic information for developing health education programs, screening, and providing appropriate solutions to remove barriers to treatment and care (12). Therefore, measuring women's knowledge is necessary for planning educational interventions regarding this disease (13).
Kashan University of Medical Sciences, covering the two cities of Kashan, Aran, and Bidgol, with a population of about half a million people in Isfahan province, has an annual incidence rate of BC of 38 per 100,000 people (14, 15). Based on the literature review, the only study conducted in this regard on women in Kashan is related to 2001. Given the many changes in age composition, literacy level, health awareness, and health intervention plans during this period, it is necessary to re-evaluate the level of knowledge and performance of women covered by this university to make necessary interventions.
2. Objectives
This study aimed to assess the knowledge, attitude, and performance of women about BC and its risk factors in patients referred to comprehensive health centers in Kashan and Aran-O-Bidgol.
3. Methods
This cross-sectional study was conducted on women with an electronic health record referring to comprehensive health centers in Kashan and Aran-O-Bidgol during 2018 - 2019. The research purpose and methodology were subjected to scrutiny by the Isfahan University of Medical Sciences (Ethics Code: IR.MUI.RESEARCH.REC.1398.322). Informed consent was obtained from all participants.
For estimating the study sample size, the performance score was defined as the primary dependent variable, and the standard deviation of the performance score was reported as 30 (16). Considering the population of more than 110,000 women above the age of 30 in the region and taking into account a drop-out rate of 20%, at least 820 random samples were studied to be able to estimate the mean performance score with 95% confidence with a maximum error of 1.5 points.
Sampling was done by stratified random sampling method. Initially, based on the information available in the health information integration system (named as SIB), the units providing health services (health base and comprehensive health service center) of the two cities were listed (Kashan: 33 units, Aran and Bidgol: 6 units). Based on the available information, 25% of the population in Aran and Bidgol and 75% of the population (out of two cities) live in Kashan; therefore, 75% of the study sample was from Kashan and 25% from Aran and Bidgol (615 participants from Kashan and 205 samples from Aran and Bidgol). Then, the units were divided according to geographical location (ie, north, south, east, west, and center), and a unit was randomly selected from each direction. Afterward, 123 participants were taken from each of the five selected units of Kashan city, and 41 participants were randomly taken from each unit of Aran and Bidgol cities.
Data were collected using a self-administered questionnaire that its content validity and reliability (alpha Cronbach) were confirmed. The Content Validity Index (CVI) of items on knowledge, attitude, and performance was 0.86, 0.96, and 1, respectively. Also, Cronbach's alpha (internal reliability) for knowledge and attitude was 0.86 and 0.68, respectively. The questionnaire has four sections, including sociodemographic and existing risk factors items, 20 items for women's knowledge of the signs and symptoms of BC, risk factors and breast self-examination, 10 items for attitude measurement, and 5 items for performance measurement. The response options for items on knowledge included "Yes", "No", and "I do not know"; with scores of 2 for Yes, 0 for No, and 1 for "I do not know". The minimum and maximum scores of knowledge were 0 and 38, respectively, which the higher score, the more the level of knowledge. Before calculating the scores of knowledge, items with opposite direction were aligned with the other items. Knowledge scoring was classified into three levels after adding the scores of each item (11 to 19 = good, 1 to 10 = moderate, and -19 to 0 = poor). Attitude items had a five-point Likert-scale response, ranging from 1 (''strongly disagree'') to 5 (''strongly agree''). Attitude scoring contained two steps. First, "strongly agree" and ''strongly disagree" responses were merged with "agree" and "disagree" responses, respectively. Then, correct answers were allocated with a score of 1, incorrect answers received a score of -1, and the answers nor agreed-nor disagreed were given a score of zero. Afterward, scores were summed up. Positive scores were classified with a good label, negative scores with a poor label, and scores of zero with a moderate label (16). Two items were used to assess performance. The first item was about the frequency of breast self-examination, and the second was about the appearance of abnormal breast symptoms during the last year. The response options of the recent item were "Yes", "No", "I do not remember". The response options of breast self-examination were "Never", "1 to 6 times a year irregularly", "7 to 11 times a year", "Monthly".
3.1. Data Analysis
Given that all of the variables were categorical, counts and percentages were used for calculations. Chi-square and Fisher's exact tests were used to compare proportions of demographic variables and risk factors across levels of knowledge, attitude, and performance. Statistical significance was considered when P-value < 0.05. Data analysis was administered using SPSS version 16.
4. Results
In this study, out of 820 participants, 776 (94.6%) completed the questionnaire correctly, of which 708 (91.2%) of them were married. In terms of age, 258 (33%) participants were under the age of 34, 381 (49%) were 35 - 39 years old, and 137 (18%) were above the age of 50. In terms of education, 243 (31.3%) had a diploma, and 247 (31.8%) hold a graduate degree.
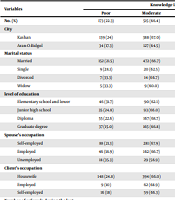
According to the findings, 88 (11.3%), 515 (66.4%), and 173 (22.3%) of the subjects had good, moderate, and poor levels of knowledge, respectively. Based on the Chi-square and Fish tests, the women’s level of knowledge in the two cities was significantly different (P < 0.001), details of which are presented in Table 1.
| Variables | Knowledge Level, No. (%) | P-Value | |||
|---|---|---|---|---|---|
| Poor | Moderate | Good | Total | ||
| No. (%) | 173 (22.3) | 515 (66.4) | 88 (11.3) | 776 (100) | |
| City | < 0.001 | ||||
| Kashan | 139 (24) | 388 (67.0) | 52 (9.0) | 579 (100) | |
| Aran-O-Bidgol | 34 (17.3) | 127 (64.5) | 36 (18.3) | 197 (100) | |
| Marital status | 0.029 | ||||
| Married | 152 (21.5) | 472 (66.7) | 84 (11.9) | 708 (100) | |
| Single | 9 (28.1) | 20 (62.5) | 3 (4.9) | 32 (100) | |
| Divorced | 7 (33.3) | 14 (66.7) | (0) | 21 (100) | |
| Widow | 5 (33.3) | 9 (60.0) | 1 (6.7) | 15 (100) | |
| level of education | < 0.001 | ||||
| Elementary school and lower | 46 (31.7) | 90 (62.1) | 9 (6.2) | 145 (100) | |
| Junior high school | 35 (24.8) | 93 (66.0) | 13 (9.2) | 141 (100) | |
| Diploma | 55 (22.6) | 167 (68.7) | 21 (8.6) | 243 (100) | |
| Graduate degree | 37 (15.0) | 165 (66.8) | 45 (18.2) | 247 (100) | |
| Spouse’s occupation | 0.076 | ||||
| Self-employed | 88 (21.3) | 281 (67.9) | 45 (1.9) | 414 (100) | |
| Employed | 46 (18.9) | 162 (66.7) | 35 (14.4) | 243 (100) | |
| Unemployed | 18 (35.3) | 29 (56.9) | 4 (7.8) | 51 (100) | |
| Client’s occupation | < 0.001 | ||||
| Housewife | 148 (24.8) | 394 (66.0) | 55 (9.2) | 597 (100) | |
| Employed | 9 (10) | 62 (68.9) | 19 (21.1) | 90 (100) | |
| Self-employed | 16 (18) | 59 (66.3) | 14 (15.7) | 89 (100) | |
| Number of referrals during the last year | 0.021 | ||||
| No referral | 37 (18.9) | 143 (73.0) | 16 (8.2) | 196 (100) | |
| Once | 95 (25.1) | 241 (63.6) | 43 (11.3) | 379 (100) | |
| 2 times | 35 (23.5) | 97 (65.1) | 17 (11.4) | 149 (100) | |
| 3 times and more | 6 (11.5) | 34 (65.4) | 12 (23.1) | 52 (100) | |
| BMI (kg/m2) | 0.019 | ||||
| Normal | 80 (27.3) | 182 (62.1) | 31 (1.6) | 293 (100) | |
| Overweight (9 / 29 - 25) | 45 (15.6) | 205 (70.9) | 39 (13.5) | 289 (100) | |
| Grade 1 obesity 99/34-30 | 26 (21.7) | 79 (65.8) | 15 (12.5) | 120 (100) | |
| Grade 2 obesity 35 and above | 10 (27.0) | 26 (70.3) | 1 (2.7) | 37 (100) | |
| Number of children | 0.804 | ||||
| None | 25 (26.9) | 59 (63.4) | 9 (9.7) | 93 (100) | |
| 1 - 3 | 136 (21.5) | 422 (66.8) | 74 (11.7) | 632 (100) | |
| 4 and more | 12 (23.5) | 34 (66.7) | 5 (9.8) | 51 (100) | |
| Breastfeeding history | 0.489 | ||||
| No | 31 (25.8) | 78 (65.0) | 11 (9.2) | 120 (100) | |
| Yes | 142 (21.6) | 437 (66.6) | 77 (11.7) | 656 (100) | |
| Breastfeeding duration (total months) | 0.902 | ||||
| Zero | 31 (25.8) | 78 (65.0) | 11 (9.2) | 120 (100) | |
| Under 23 | 26 (2.3) | 89 (69.5) | 13 (1.2) | 128 (100) | |
| 24 - 59 | 98 (21.8) | 297 (66.1) | 54 (12.0) | 449 (100) | |
| Over 60 | 18 (22.8) | 51 (64.6) | 10 (12.7) | 79 (100) | |
| Menopause status | 0.15 | ||||
| Having menstrual cycle | 139 (21.4) | 431 (66.4) | 79 (12.2) | 649 (100) | |
| Menopausal | 34 (26.8) | 84 (66.1) | 9 (7.1) | 127 (100) | |
| Menopausal age (y) | 0.23 | ||||
| 53 and low | 32 (28.3) | 72 (63.7) | 9 (8.0) | 113 (100) | |
| 54 and above | 2 (14.3) | 12 (85.7) | 0 (.0) | 14 (100) | |
| Age of first menstruation (y) | 0.775 | ||||
| Under 11 | 26 (25.2) | 68 (66.0) | 9 (8.7) | 103 (100) | |
| 11 - 15 | 134 (21.5) | 415 (66.6) | 74 (11.9) | 623 (100) | |
| Above 16 years | 13 (26.0) | 32 (64.0) | 5 (1.0) | 50 (100) | |
Level of Knowledge of Breast Cancer in Terms of Demographic Variables and Risk Factors
There was a significant relationship between the level of knowledge and some of the variables, such as marital status (P = 0.029), level of education (P < 0.001), Client’s occupation (P < 0.001), and the number of referrals during the last year (P = 0.021). Moreover, there was a significant relationship between the level of knowledge with body mass index (P = 0.019). However, there was no significant relationship between the level of knowledge with spouse’s occupation, the number of children, history of breastfeeding, menopausal status, menopausal age, age of first menstruation, and family history of BC (P > 0.05) (Table 1).
There was a significant relationship between attitude score with spouse’s age and occupation. Moreover, 86 (11.1%), 595 (76.7%), and 95 (12.2%) participants had poor, moderate, and good attitude toward cancer risk factors (Table 2).
| Variables | Attitude Level, No. (%) | P-Value | |||
|---|---|---|---|---|---|
| Poor | Moderate | Good | Total | ||
| No. (%) | 86 (11.1) | 595 (76.7) | 95 (12.2) | 776 (100) | |
| City | 0.926 | ||||
| Kashan | 63 (10.9) | 444 (76.7) | 72 (12.4) | 579 (100) | |
| Aran-O-Bidgol | 23 (11.7) | 151 (76.6) | 23 (11.7) | 197 (100) | |
| Age (y) | 0.003 | ||||
| Under 34 | 33 (12.8) | 201 (77.9) | 24 (9.3) | 258 (100) | |
| 35 - 49 | 32 (8.4) | 287 (75.3) | 62 (16.3) | 381 (100) | |
| Above 50 | 21 (15.3) | 107 (78.1) | 9 (6.6) | 137 (100) | |
| Education level | 0.1 | ||||
| Elementary school and lower | 20 (13.8) | 104 (71.7) | 21 (14.5) | 145 (100) | |
| Junior high school | 10 (7.1) | 112 (79.4) | 19 (13.5) | 141 (100) | |
| Diploma | 27 (11.1) | 180 (74.1) | 36 (14.8) | 243 (100) | |
| Graduate degree | 29 (11.7) | 199 (80.6) | 19 (7.7) | 247 (100) | |
| Income (million Toman) | 0.016 | ||||
| Under one | 14 (8.9) | 115 (73.2) | 28 (17.8) | 157 (100) | |
| From 1.5 - 2 | 27 (11.2) | 187 (77.6) | 27 (11.2) | 241 (100) | |
| From 2 - 3 | 16 (14.0) | 85 (74.6) | 13 (11.4) | 114 (100) | |
| From 3 and above | 5 (19.2) | 19 (73.1) | 2 (7.7) | 26 (100) | |
| Spouse’s occupation | 0.005 | ||||
| Self-employed | 45 (10.9) | 314 (75.8) | 55 (13.3) | 414 (100) | |
| Employed | 20 (8.2) | 197 (81.1) | 26 (10.7) | 243 (100) | |
| Unemployed | 13 (25.5) | 31 (60.8) | 7 (13.7) | 51 (100) | |
The Subjects’ Attitude Level in Terms of Demographic Variables of Breast Cancer
According to Table 3, there was a significant relationship between age, marital status, education level, and income with the performance of breast self-examination (P < 0.05). The married people had more breast self-examination than single people, and by increasing education level, age and income, more breast self-examination was observed.
| Variables | Breast Self-examination, No. (%) | P-Value | |||
|---|---|---|---|---|---|
| Never | 1 to 6 Times a Year Irregularly | 7 to 11 Times a Year | Monthly | ||
| Total | 341 (43.9) | 330 (42.5) | 35 (4.5) | 70 (9.0) | |
| City | 0.26 | ||||
| Kashan | 261 (45.1) | 247 (42.7) | 22 (3.8) | 49 (8.5) | |
| Aran-O-Bidgol | 80 (40.6) | 83 (42.1) | 13 (6.6) | 21 (10.7) | |
| Age (y) | < 0.001 | ||||
| Under 34 | 142 (55.0) | 84 (32.6) | 8 (3.1) | 24 (9.3) | |
| 35 - 49 | 165 (43.3) | 160 (42.0) | 19 (5.0) | 37 (9.7) | |
| Above 50 | 34 (24.8) | 86 (62.8) | 8 (5.8) | 9 (6.6) | |
| Marital status | 0.031 | ||||
| Married | 304 (42.9) | 309 (43.6) | 30 (4.2) | 65 (9.2) | |
| Single | 22 (68.8) | 6 (18.8) | 1 (3.1) | 3 (9.4) | |
| Divorced | 11 (52.4) | 7 (33.3) | 3 (14.3) | 0 (0.0) | |
| Widow | 4 (26.7) | 8 (53.3) | 1 (6.7) | 2 (13.3) | |
| Education level | 0.003 | ||||
| Elementary school and lower | 54 (37.2) | 77 (53.1) | 8 (5.5) | 6 (4.1) | |
| Junior high school | 63 (44.7) | 59 (41.8) | 8 (5.7) | 11 (7.8) | |
| Diploma | 113 (46.5) | 105 (43.2) | 9 (3.7) | 16 (6.6) | |
| Graduate degree | 111 (44.9) | 89 (36.0) | 10 (4.0) | 37 (15.0) | |
| Income (million Toman) | 0.026 | ||||
| Under one | 75 (47.8) | 57 (36.3) | 14 (8.9) | 11 (7.0) | |
| From 1.5 - 2 | 85 (35.3) | 120 (49.8) | 11 (4.6) | 25 (10.4) | |
| From 2 - 3 | 51 (44.7) | 43 (37.7) | 4 (3.5) | 16 (14.0) | |
| From 3 and above | 9 (34.6) | 11 (42.3) | 1 (3.8) | 5 (19.2) | |
Frequency of Breast Self-examination in Terms of Demographic Variables
The findings indicated that 134 (23.7%) subjects observed abnormal breast symptoms. Moreover, there was a significant relationship between observing abnormal breast symptoms with the variables of city, age, and income. There was a significant relationship between performance in observing abnormal breast symptoms and variables of the number of children, breastfeeding history, breastfeeding duration, menopause status, and age of first menstruation (Table 4).
| Variables | Observing Abnormal Breast Symptoms, No. (%) | P-Value | ||
|---|---|---|---|---|
| Yes | No | I Do Not Remember | ||
| Total | 134 (23.7) | 511 (65.8) | 81 (10.4) | |
| City | 0.005 | |||
| Kashan | 154 (26.6) | 368 (63.6) | 57 (9.8) | |
| Aran-O-Bidgol | 30 (15.2) | 143 (72.6) | 24 (12.2) | |
| Age (y) | 0.03 | |||
| Under 34 | 48 (18.6) | 181 (70.2) | 29 (11.2) | |
| 35 - 49 | 91 (23.9) | 248 (65.1) | 42 (11.0) | |
| Above 50 | 45 (32.8) | 82 (59.9) | 10 (7.3) | |
| Income (million Toman) | 0.012 | |||
| Under 1 | 31 (19.7) | 106 (67.5) | 20 (12.7) | |
| From 1.5 - 2 | 76 (31.5) | 144 (59.8) | 21 (8.7) | |
| From 2 - 3 | 19 (16.7) | 82 (71.9) | 13 (11.4) | |
| From 3 and above | 9 (34.6) | 17 (65.4) | 0 (0.0) | |
| Spouse’s occupation | 0.012 | |||
| Self-employed | 89 (21.5) | 279 (67.4) | 46 (11.1) | |
| Employed | 59 (24.3) | 161 (66.3) | 23 (9.5) | |
| Unemployed | 22 (43.1) | 27 (52.9) | 2 (3.9) | |
| Number of children | 0.008 | |||
| None | 8 (8.6) | 72 (77.4) | 13 (14.0) | |
| 1 - 3 | 163 (25.8) | 407 (64.4) | 62 (9.8) | |
| 4 and more | 13 (25.5) | 32 (62.7) | 6 (11.8) | |
| Breastfeeding history | 0.012 | |||
| No | 16 (13.3) | 88 (73.3) | 16 (13.3) | |
| Yes | 168 (25.6) | 423 (64.5) | 65 (9.9) | |
| Breastfeeding duration (total months) | 0.009 | |||
| Zero | 16 (13.3) | 88 (73.3) | 16 (13.3) | |
| Under 23 | 25 (19.5) | 86 (67.2) | 17 (13.3) | |
| 24 - 59 | 124 (27.6) | 289 (64.4) | 36 (8.0) | |
| Over 60 | 19 (24.1) | 48 (60.8) | 12 (15.2) | |
| Menopause status | 0.013 | |||
| Having menstrual cycle | 142 (21.9) | 434 (66.9) | 73 (11.2) | |
| Menopausal | 42 (33.1) | 77 (60.6) | 8 (6.3) | |
| Age of first menstruation (y) | 0.039 | |||
| Under 11 | 30 (29.1) | 60 (58.3) | 13 (12.6) | |
| 11 - 15 | 149 (23.9) | 409 (65.7) | 65 (1.4) | |
| Above 16 | 5 (1.0) | 42 (84.0) | 3 (6.0) | |
Frequency of Performance Score in Observing Abnormal Breast Symptoms Based on Demographic Variables and Risk Factors
There was a significant relationship between performance score with the number of breast self-examination and variables of the number of children, breastfeeding history, breastfeeding duration, menopausal status, and the number of referrals (Table 5).
| Variables | Breast Self-examination, No. (%) | P-Value | |||
|---|---|---|---|---|---|
| Never | 1 to 6 Times a Year Irregularly | 7 to 11 Times a Year | Monthly | ||
| Total | Total | 341 (43.9) | 330 (42.5) | 35 (4.5) | |
| City | 0.26 | ||||
| Kashan | 261 (45.1) | 247 (42.7) | 22 (3.8) | 49 (8.5) | |
| Aran-O-Bidgol | 80 (40.6) | 83 (42.1) | 13 (6.6) | 21 (10.7) | |
| Number of children | 0.001 | ||||
| None | 59 (63.4) | 21 (22.6) | 3 (3.2) | 10 (10.8) | |
| 1 - 3 | 267 (42.2) | 281 (44.5) | 30 (4.7) | 54 (8.5) | |
| 4 and more | 15 (29.4) | 28 (54.9) | 2 (3.9) | 6 (11.8) | |
| Breastfeeding history | 0.002 | ||||
| No | 70 (58.3) | 33 (27.5) | 4 (3.3) | 13 (10.8) | |
| Yes | 271 (41.3) | 297 (45.3) | 31 (4.7) | 57 (8.7) | |
| Breastfeeding duration (total months) | < 0.001 | ||||
| Zero | 70 (58.3) | 33 (27.5) | 4 (3.3) | 13 (10.8) | |
| Under 23 | 64 (50.0) | 47 (36.7) | 4 (3.1) | 13 (10.2) | |
| 24 - 59 | 181 (40.3) | 218 (48.6) | 20 (4.5) | 30 (6.7) | |
| Over 60 | 26 (32.9) | 32 (40.5) | 7 (8.9) | 14 (17.7) | |
| Menopause status | < 0.001 | ||||
| Having menstrual cycle | 309 (47.6) | 251 (38.7) | 28 (4.3) | 61 (9.4) | |
| Menopausal | 32 (25.2) | 79 (62.2) | 7 (5.5) | 9 (7.1) | |
| Number of referrals (during the last year) | < 0.001 | ||||
| No referral | 100 (51.0) | 63 (32.1) | 14 (7.1) | 19 (9.7) | |
| Once | 161 (42.5) | 182 (48.0) | 11 (2.9) | 25 (6.6) | |
| 2 times | 59 (39.6) | 68 (45.6) | 4 (2.7) | 18 (12.1) | |
| 3 times and more | 21 (40.4) | 17 (32.7) | 6 (11.5) | 8 (15.4) | |
Frequency of Breast Self-examination in Terms of Risk Factors
The highest correlation coefficient was found between the status of knowledge and attitude of women toward BC, but the linear correlation coefficient between attitude and knowledge as well as attitude and performance were -0.072 and -0.052, respectively.
5. Discussion
This study showed that more than half of the participants had a moderate level of knowledge and attitude about the signs, symptoms, and risk factors for breast cancer and the correct method of self-examination and clinical examination of the breast. The results indicated that only 11% of the participants had a good level of knowledge. A good level of knowledge was significantly higher in married, graduated, and employed women. Those with a good level of knowledge had a higher number of referrals during the last year. Also, the findings showed that 12% of the participants had a good level of attitude. The women with an age range of 35 to 49 and those who were self-employed had a higher level of attitude.
According to the findings, most women had irregular breast self-examination. The women who were under 34 years of age, single, and graduated had the lowest irregular frequency of breast self-examination, which may indicate their high-risk perception.
The results of the present study are consistent with those of Godazandeh and Jorgensen, who reported that about 2.3% of the Iranian women had a moderate to low level of this knowledge, and it seems that they have less knowledge of the benefits of BC screening when they have no symptoms (17). Montazeri et al., in 2002, reported that the level of knowledge and attitude of health workers was moderate, and implementing educational programs related to cancer prevention was recommended for this group (18). Although mammography is more sensitive in the early diagnosis of BC, compared to clinical breast examination, most research institutions in the world, perform a clinical breast examination and mammography together following a specific screening program in women aged above 20 years, especially those older than 40 years (1, 19). Nevertheless, regular breast self-examination can, in addition to helping in the early diagnosis of the disease, improve the level of knowledge and attitude of the community towards cancer and its prevention methods (20, 21).
Accordingly, education has an effective role in advancing community health promotion. By educating the community regarding the correct implementation of prevention programs, the level of their knowledge and attitude about BC increases, leading to the implementation of more prevention and screening programs for BC, as well as the implementation of educational programs related to women. A study conducted in the southern coast of the Caspian Sea mentioned that lack of intervention programs for health education in Iranian society and lack of regular community-based screening programs have reduced the level of knowledge and attitude towards BC. Therefore, there was a significant decrease in the level of acceptance of Iranian women even at high levels of education in the implementation of BC prevention programs, especially clinical breast examination and mammography (22). Similar results have been observed in studies conducted in other countries (23, 24).
These results are in line with the studies by Tawafian et al. (25), Montazeri et al. (18), and Jervandi et al. (26), which indicated that low economic and social status, low level of education, and lack of knowledge about BC and breast self-examination are the most important reasons for low breast self-examination. However, in several studies, including Haririchi et al. (27), Peerson and Saunders (13), Arndt et al. in Germany (28), Huo et al. in China (29), and Mirfarhadi et al. (30), a strong relationship was observed between the disease and referral time. According to these studies, the mortality rate of this cancer over the past 30 years, despite technical advances in surgery, chemotherapy, and radiotherapy, has been constant due to the referral of most patients in the advanced stages of the disease. Similar studies have shown that low levels of education and income are among factors affecting patients' referral in the advanced stages of the disease (27, 28, 30).
The results of this study indicated the need for paying more attention to increasing women's knowledge about the risk factors of BC and effective screening methods. Due to the high burden of cancer in the region and the referral of patients in the advanced stages of the disease, it is necessary to organize and implement a well-organized educational program for the public and establish facilities for mammography every three years for those aged above 40. In addition, another important measure would be expanding health insurance coverage to diagnostic and therapeutic examinations.
Breast self-examination is the easiest and cheapest way for early diagnosis of the disease and is the only method of BC screening for women who do not have sufficient access to health care (31). In the present study, 9.05% of the subjects regularly performed breast self-examination.
Various studies suggested that improving public knowledge and attitude toward BC can play a positive role in screening behaviors of women in the community (32-34). Comparing the results of different studies with those of the present study revealed a significant similarity between breast self-examinations in developing countries, which is very different from that of developed ones. These results indicate that, among other factors, cultural similarities or differences may have a significant contribution to such differences. The study population had a moderate to poor level of knowledge about BC prevention and screening programs. However, they had a positive attitude toward BC prevention and screening programs.
Considering the high level of education in the Iranian women's community, in comparison with other developing countries in Central Asia, the Middle East, the Caucasus, Africa, and Latin America, it seems that designing and implementing health education interventional programs on cancer, especially BC, will increase the effectiveness of BC screening programs among the Iranian women's community compared to other countries.
It is necessary to mention some limitations of our study, including using self-administered questionnaires to collect data, which is prone to measurement bias. Following a cross-sectional design, which does not allow to make any causal inference about the association between performance and knowledge and attitude. Last but not least, this study was conducted on only women with electronic health records in comprehensive health centers in Kashan and Aran-O-Bidgol, which limits its generalizability.
5.1. Conclusions
Given the low level of knowledge, attitude, and performance of older women with low education levels, as well as increasing the risk of the disease in the elderly, it is necessary to perform educational interventions appropriate for this age group. In addition, given the importance of early detection in breast cancer, training programs intended to update the knowledge about its risk factors and those intended to promote breast cancer screening practice in healthcare centers can potentially improve women's practice of healthy habits.
