




1. Background
Social anxiety disorder (SAD) represents a significant mental health challenge among university students, affecting various aspects of their academic and social lives (1). The transition to higher education exposes students to numerous social situations and academic demands, which can exacerbate symptoms of SAD (2). Social anxiety disorder is characterized by an intense fear of negative evaluation in social contexts, severely impacting the well-being and functioning of affected individuals (3). From participating in class discussions to attending social gatherings, students with SAD often experience overwhelming anxiety and distress, leading to avoidance behaviors and impairment in daily functioning (4). In Iran, a study involving 29,878 participants identified 585 individuals with SAD, resulting in a lifetime weighted prevalence of 1.8% (5).
Social anxiety disorder and depression are two prevalent mental health conditions that frequently co-occur, significantly impacting individuals' lives (6). Both disorders can vary in severity, from mild to severe, and can impair social, occupational, and academic functioning (7). Although SAD and depression are distinct disorders, they often coexist, with research indicating a high rate of comorbidity between the two (8). Individuals with SAD may develop symptoms of depression due to the chronic stress and isolation associated with their social anxiety, while those with depression may develop SAD as a result of negative self-perception and withdrawal from social interactions (9). Individuals with both disorders may experience greater functional impairment and increased emotional problems compared to those with only one of the disorders (10). Emotion regulation, on the other hand, refers to the ability to monitor, evaluate, and modulate one's emotional experiences and expressions in response to internal and external stimuli (11). Various factors contribute to the relationship between SAD and emotion regulation, including underlying neurobiological processes, cognitive biases, and environmental stressors (12). Additionally, negative self-beliefs and early life experiences may shape individuals' emotion regulation strategies, contributing to the development of SAD (13). Individuals grappling with SAD often struggle to regulate their emotions effectively, leading to heightened emotional reactivity and maladaptive coping strategies (14). SAD and self-concept are two psychological constructs that significantly influence individuals' perceptions of themselves and their interactions with the world around them (15). Self-concept refers to the beliefs, perceptions, and evaluations individuals hold about themselves, including their abilities, traits, and worth (16). Individuals with SAD often experience negative beliefs and evaluations about themselves, which can profoundly impact their self-concept (17). These individuals may perceive themselves as socially inept, unlikable, or unworthy of acceptance and approval from others (18). Research suggests a bidirectional relationship between SAD and self-concept, with each influencing and exacerbating the other over time (19). Conversely, the experience of social anxiety can further undermine self-concept, reinforcing negative beliefs about oneself and perpetuating a cycle of self-doubt and avoidance (20).
Metacognitive therapy (MCT) offers a unique approach by focusing on the regulation of metacognitive processes, such as rumination, worry, and cognitive biases, which contribute to the maintenance of SAD (21). Metacognitive therapy aims to challenge unhelpful cognitive processes and promote adaptive metacognitive strategies that facilitate effective emotion regulation and problem-solving (22). By encouraging students to develop an awareness of their thinking patterns and adopt flexible coping strategies, MCT empowers individuals to manage SAD more effectively and improve their mental health (23). Research into the effectiveness of MCT for students with SAD has shown promising results (24). Studies have indicated significant reductions in SAD symptoms, improvements in emotion regulation, and enhanced self-concept among participants who underwent MCT (25). Importantly, these benefits appear to be sustained over time, with individuals reporting long-term improvements in their ability to manage social anxiety triggers and participate more actively in academic and social activities (26). Nordahl and Wells found that symptoms continued to decrease even six months post-treatment, suggesting lasting therapeutic effects (27). In a study by Lakshmi et al. (28), it was found that MCT was more effective than applied relaxation in reducing social avoidance, post-event processing, and self-consciousness.
2. Objectives
This study aims to assess the efficacy of MCT in students diagnosed with SAD. Specifically, the study seeks to evaluate the impact of MCT on reducing SAD symptoms, improving emotion regulation, and enhancing self-concept among students with SAD.
3. Methods
3.1. Study Design
The current study utilized a quasi-experimental research design, incorporating a pre-test-post-test structure with a control group.
3.2. Study Population and Sampling
The study focused on students with SAD enrolled at the University of Tehran in 2022. To recruit participants, invitations were initially sent to various student groups. From an initial pool of 78 students assessed, 36 individuals who scored above 40 on the Liebowitz Social Anxiety Scale (LSAS) were selected as the final sample. These 36 students were then randomly allocated, via a lottery system, into either the experimental group (n = 18) or the control group (n = 18). The sample size of 36 was determined using G*Power software, taking into account factors relevant to the analysis of covariance (29). Inclusion criteria included being a member of the research community, having no reported physical issues, a willingness to participate, and proficiency in reading and writing. Additionally, missing more than two sessions or expressing unwillingness to continue participation were considered grounds for withdrawal from the study.
3.3. Tools
3.3.1. The Liebowitz Social Anxiety Scale
The LSAS consists of 24 items, with 11 items assessing fear and 13 items assessing avoidance across various social situations such as public speaking, initiating conversations, and eating in public (30). Each item on the LSAS is rated on a Likert scale ranging from 0 to 3, where 0 indicates "none" or "never fear/avoid," and 3 indicates "severe" or "always fear/avoid." The total score can range from 0 to 72, with higher scores indicating more pronounced levels of social anxiety. In the present study, the Cronbach's alpha coefficient for this scale was determined to be 0.91, indicating high internal consistency.
3.3.2. The Beck Depression Inventory (BDI)
The BDI is a widely used self-report questionnaire designed to assess the severity of depression symptoms in individuals aged 13 and older (31). It consists of 21 multiple-choice items, each corresponding to a specific symptom of depression. Scores for each item range from 0 to 3, with a total score ranging from 0 to 63. Beck et al. (31) reported the validity of the test as 0.96, with internal consistency ranging from 0.73 to 0.92 and a mean of 0.86. In the current study, the Cronbach's alpha coefficient for this scale was calculated and found to be 0.82.
3.3.3. The Emotion Regulation Questionnaire (ERQ)
The ERQ is a self-report measure developed by Gross and John (32) to assess individual differences in emotion regulation strategies (32). It comprises 10 items, with six items assessing cognitive reappraisal and four items assessing expressive suppression. Participants indicate the degree to which they utilize each strategy using a Likert scale, typically ranging from 1 (strongly disagree) to 7 (strongly agree). In the study by Gross and John (32), internal correlation coefficients of 0.79 for the cognitive reappraisal subscale and 0.73 for the expressive suppression subscale were documented. In the current study, Cronbach's alpha coefficients for the cognitive reappraisal and expressive suppression subscales were determined to be 0.89 and 0.84, respectively.
3.3.4. The Beck Self-concept Test (BSCT)
Developed in 1990 by Beck et al. (16), the scale comprises 25 items evaluated on a Likert scale, ranging from 1 (low) to 5 (high). The Cronbach's alpha coefficient was calculated to be 0.82, indicating good internal consistency. The retest reliability over one week and three months was reported as 0.88 and 0.65, respectively. Additionally, the internal consistency coefficient for this scale was reported as 0.80 (16). In the current study, the Cronbach's alpha coefficient of this questionnaire was determined to be 0.89.
3.4. Intervention Procedure
Following the pre-test phase, the experimental group participated in a series of ten 90-minute training sessions of MCT based on the Wells model (21). These sessions were conducted once a week over three months. After completing the intervention, both the experimental and control groups were reassessed during the post-test phase. The MCT intervention was administered by the researcher in 2022, following all health protocols, at a psychological services clinic. At the beginning of each session, homework from the previous session was reviewed, and participants received constructive feedback (Table 1) (21).
| Sessions | Topic |
|---|---|
| 1 | Welcome, discussion about the venue, number of sessions, duration, and duration of each session, bringing up the rules and regulations of the group, introducing and familiarizing the members, explaining the research tools, and completing the questionnaires by the participants. |
| 2 | Summarizing the content of the previous session with the help of the members, explaining what the metacognitive model is, dissociative mindfulness techniques, teaching attention and postponing worry, and presenting its diagram, presenting the assignment and emphasizing completing the assignment, receiving feedback. |
| 3 | Discussion about positive metacognitive beliefs and negative metacognitive beliefs and their practice, teaching the technique of broken mindfulness, and testing the suppression-non-suppression practice of the technique of postponing focused attention on uncontrollable beliefs. |
| 4 | Receiving feedback from the previous session, reviewing the exercise and assignment of the previous session (example of positive and negative metacognitive beliefs), challenging with positive and negative metacognitive beliefs, teaching the technique of postponing worry, training and practicing the technique of metacognitive guidance |
| 5 | We are receiving feedback from the previous session, discussing homework, teaching and practicing free association, presenting homework, and receiving feedback. |
| 6 | Using the technique of confronting and preventing the response focused on reassuring beliefs, the technique of refocusing attention on safety signs, teaching and practicing the anti-inhibition test, and providing homework. |
| 7 | We are receiving feedback from the previous session, reviewing homework, teaching and practicing the technique of prescribing the wandering mind, teaching tiger assignment practice, presenting assignments, and receiving feedback. |
| 8 | Teaching the technique of making changes in threat monitoring focused on self-awareness beliefs, using verbal and behavioral re-documentation techniques focused on risk beliefs. |
| 9 | We are receiving feedback from the previous session, reviewing homework, teaching and practicing the verbal loop technique, teaching the practice of the rebellious child technique, presenting the assignment, receiving feedback, and answering the questions raised by the members. |
| 10 | Training in the technique of examining opposing evidence and preparing members to identify the obstacles in using the techniques and finally conclude. |
Summary of Metacognitive Therapy Sessions
3.5. Statistical Analysis
The research data were analyzed using descriptive statistics, including mean and standard deviation, along with covariance analysis, adhering to the assumptions of the analysis. SPSS-24 software was utilized for this purpose. The significance level for these tests was set at 0.05.
4. Results
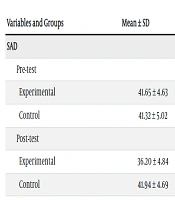
The mean and standard deviation of age for the experimental group were 26.41 ± 5.35, while for the control group, they were 26.38 ± 4.26. Table 2 presents the mean and standard deviation of the pre-test and post-test scores for depression, cognitive reappraisal, expressive suppression, and self-concept in students with SAD within both the experimental and control groups.
| Variables and Groups | Mean ± SD | S-W | P |
|---|---|---|---|
| SAD | |||
| Pre-test | |||
| Experimental | 41.65 ± 4.63 | 0.103 | 0.072 |
| Control | 41.32 ± 5.02 | 0.075 | 0.051 |
| Post-test | |||
| Experimental | 36.20 ± 4.84 | 0.113 | 0.059 |
| Control | 41.94 ± 4.69 | 0.096 | 0.065 |
| Depression | |||
| Pre-test | |||
| Experimental | 26.83 ± 1.68 | 0.057 | 0.061 |
| Control | 26.80 ± 1.69 | 0.102 | 0.072 |
| Post-test | |||
| Experimental | 23.72 ± 2.58 | 0.093 | 0.065 |
| Control | 29.94 ± 1.69 | 0.056 | 0.097 |
| Cognitive reappraisal | |||
| Pre-test | |||
| Experimental | 28.50 ± 2.83 | 0.059 | 0.068 |
| Control | 28.27 ± 2.86 | 0.074 | 0.054 |
| Post-test | |||
| Experimental | 31.83 ± 3.01 | 0.061 | 0.093 |
| Control | 28.49 ± 2.20 | 0.097 | 0.074 |
| Pre-test | |||
| Experimental | 16.94 ± 1.89 | 0.075 | 0.058 |
| Control | 16.72 ± 2.78 | 0.119 | 0.067 |
| Post-test | |||
| Experimental | 19.88 ± 2.60 | 0.093 | 0.084 |
| Control | 16.27 ± 2.21 | 0.084 | 0.083 |
| Pre-test | |||
| Experimental | 70.16 ± 3.16 | 0.075 | 0.075 |
| Control | 70.28 ± 3.28 | 0.093 | 0.062 |
| Post-test | |||
| Experimental | 73.94 ± 3.45 | 0.134 | 0.067 |
| Control | 70.50 ± 3.43 | 0.063 | 0.051 |
Descriptive Measures of Study Variables in Control and Experimental Groups
The study employed multivariate analysis of covariance (MANCOVA) to investigate the impact of MCT on depression, cognitive reappraisal, expressive suppression, and self-concept among students with SAD. The researchers ensured that the assumptions regarding variance equality, the covariance matrix, and regression coefficients were met before proceeding with the analysis. The results (Wilks' Lambda = 0.227, F = 23.04, P < 0.001, η² = 0.76) indicated significant effects of the independent variable (MCT) on the dependent variables. Following this, group differences for each variable were further explored using one-way analysis of variance (ANOVA), with the detailed results presented in Table 3.
| Variables | SS | SS Error | DF | MS | MS Error | F | P-Value | Effect Value |
|---|---|---|---|---|---|---|---|---|
| Depression | 97.084 | 57.49 | 1 | 97.084 | 1.91 | 50.65 | 0.001 | 0.63 |
| Cognitive reappraisal | 115.650 | 56.12 | 1 | 115.650 | 1.87 | 61.81 | 0.001 | 0.67 |
| Expressive suppression | 92.700 | 80.11 | 1 | 92.700 | 2.67 | 34.72 | 0.001 | 0.54 |
| Self-concept | 104.751 | 64.75 | 1 | 104.751 | 2.15 | 48.53 | 0.001 | 0.62 |
Univariate Analysis of Covariance Results for Mean Post-Test Scores of Dependent Variables in Experimental and Control Groups
Based on the information provided in Table 3, the F-statistic for depression (F = 50.65), cognitive reappraisal (F = 61.81), expressive suppression (F = 34.72), and self-concept (F = 48.53) is significant at the 0.001 level. These results indicate a substantial difference between the experimental and control groups concerning these variables. Furthermore, the calculated effect sizes show that 63% of the variance in depression, 67% in cognitive reappraisal, 54% in expressive suppression, and 62% in self-concept can be attributed to the effect of the MCT. Therefore, it can be concluded that MCT significantly reduces depression while enhancing cognitive reappraisal, expressive suppression, and self-concept in students diagnosed with SAD.
5. Discussion
The primary aim of this study is to assess the effectiveness of MCT in addressing depression, enhancing emotion regulation skills, and fostering self-concept among students diagnosed with SAD. The findings from this research offer significant insights into the efficacy of MCT in mitigating symptoms of depression among students grappling with SAD. The observed reduction in depression levels following MCT intervention underscores the potential therapeutic benefits of this approach for addressing the psychological distress experienced by students with SAD (21).
The significant decrease in depression levels among students with SAD following MCT intervention aligns with previous research highlighting the role of cognitive-behavioral interventions in treating comorbid conditions such as depression in individuals with SAD (4). Metacognitive therapy targets maladaptive metacognitive processes, such as rumination and worry, which are often implicated in the maintenance of depressive symptoms (23). By challenging negative thought patterns and promoting adaptive coping strategies, MCT may help students with SAD develop more resilient cognitive frameworks and reduce their vulnerability to depressive episodes (8). Furthermore, the observed decrease in depression levels may be attributed to improvements in emotion regulation skills among students participating in MCT (22).
The outcomes of the present study provide compelling evidence supporting the positive impacts of MCT on enhancing emotion regulation skills among students diagnosed with SAD. Specifically, the observed improvements in cognitive reappraisal and expressive suppression following MCT intervention highlight the potential of this therapeutic approach to enhance emotion regulation abilities in individuals grappling with SAD (14). The significant increase in cognitive reappraisal among students with SAD after receiving MCT aligns with the theoretical underpinnings of this intervention (11). Metacognitive therapy aims to target maladaptive metacognitive processes, such as rumination and worry, which often contribute to heightened emotional reactivity and impaired emotion regulation (28). By encouraging individuals to adopt a more flexible and adaptive cognitive perspective on their emotional experiences, MCT may empower students with SAD to reinterpret social situations in less threatening ways, thereby facilitating cognitive reappraisal as a coping strategy (21). Similarly, the observed increase in expressive suppression among students with SAD following MCT intervention underscores the therapeutic benefits of this approach in promoting adaptive emotion regulation strategies (25).
The findings of the present study provide compelling evidence for the positive impact of MCT on self-concept among students diagnosed with SAD. The observed improvement in self-concept following MCT intervention highlights the potential of this therapeutic approach to foster a more positive self-perception and enhance overall well-being in individuals grappling with SAD (22). Metacognitive therapy aims to target maladaptive metacognitive processes, such as negative self-beliefs and self-critical rumination, which often contribute to low self-esteem and negative self-concept in individuals with SAD (20). By challenging distorted self-perceptions and promoting adaptive self-reflection, MCT may empower students with SAD to develop a more accurate and positive sense of self (28). The improvement in self-concept observed in students with SAD following MCT intervention has important implications for their psychological well-being and social functioning (17). A positive self-concept is associated with greater resilience, self-efficacy, and interpersonal relationships, all of which are critical for navigating social interactions and achieving academic success (21). By fostering a more favorable self-concept, MCT may help students with SAD overcome feelings of inadequacy and insecurity, cultivating a greater sense of confidence and self-worth (27).
5.1. Conclusions
The results of this study provide valuable insights into the therapeutic benefits of MCT for students affected by SAD. Metacognitive therapy targets critical psychological areas such as depression, emotion regulation, and self-concept, offering the potential to significantly improve the well-being and functionality of students with SAD. These findings underscore the importance of implementing evidence-based interventions to support the mental health and academic success of these students. Moreover, this study enhances our understanding of the effectiveness of MCT in addressing the complex challenges faced by students with SAD. By fostering improvements in depression, emotion regulation, and self-concept, MCT has the potential to empower students to lead more fulfilling and resilient lives. These findings have significant implications for developing tailored interventions that specifically address the intricate relationship between SAD and psychological well-being among students facing mental health challenges.
