We evaluated the serum levels of vitamins C, D, and E in an Iranian cohort that had previously been vaccinated against COVID-19 but experienced disease relapse. Our findings suggest that these vitamins, either individually or in combination, significantly influence the recurrence of infection and the clinical status of the disease. Previous research has recognized the profound impact of an individual's nutritional status on the immune system, which can lead to altered immune responses, an increased risk of infection, and disease severity (
15). Several clinical trials have indicated the potential benefits of micronutrient supplementation, including vitamins and minerals, in the management of COVID-19 patients (
4).
Our results unequivocally demonstrate a decrease in the levels of vitamins C, D, and E among ICU patients with COVID-19. Furthermore, we observed substantial deficiencies in combinations of these vitamins among ICU patients compared to other groups (
Figure 1 and
Table 2). Consuming foods rich in vitamins C, D, and E, as well as minerals like zinc, can lead to a healthier lifestyle and enhanced immunity against diseases caused by bacteria, viruses, and parasites. Some studies have suggested that flavonoids may have the potential to inhibit the transmission of COVID-19.
There is a substantial body of evidence, both from animal studies and clinical trials, supporting the beneficial effects of antioxidant vitamins C and E on the immune response, involving both innate and adaptive pathways. These vitamins contribute to resistance against and treatment of both respiratory and systemic infections (
16,
17). Nevertheless, the use of vitamin C in the treatment of COVID-19 patients remains a topic of controversy (
18-
20). Lee and Man-Fan Wan proposed the necessity of vitamin E in the proliferation of total T and T-helper cells in Asians (
21). However, variations in human results may be attributed, at least in part, to pro-inflammatory cytokine gene polymorphisms (
22). Vitamin E has been shown to play a crucial role in counteracting the oxidative stress induced by viral infections and in protecting against lung and liver damage (
23).
The immunomodulatory effects of vitamin D and its supportive role in COVID-19 have been extensively demonstrated through various mechanisms (
24-
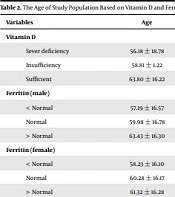
26). Sex hormones play a role in maintaining 25(OH)D levels through hormone metabolism pathways. In this context, the association of low sex hormone-binding globulin (SHBG), high luteinizing hormone, and high normal testosterone (T)/estradiol (E2) ratio with more significance in the elderly has been demonstrated (
27-
29). Consequently, we assessed the relationship between vitamin D levels and age in individuals above and below 50, revealing no significant correlation between vitamin D status and age.
Vitamins C and D are often prescribed together due to their combined benefits in supporting the immune system. Previous studies have underscored the importance of evaluating vitamins and trace elements, particularly vitamins C, D, and selenium, in COVID-19 patients (
30). In our study, we identified a significant deficiency of vitamins C and D in patients compared to the control group, and this deficiency was proportional to the severity of the disease. Several studies have established a connection between the severity of COVID-19 and vitamin D deficiency, along with elevated levels of anti-SARS-CoV-2 IgGs. The synergistic effects of other vitamins, such as thiamine derivatives in combination with ascorbic acid, in the context of COVID-19 and other viral infections remain fully understood (
31,
32). Adequate levels of vitamins C, D, and E, in conjunction with other vitamins and minerals, have been emphasized to alleviate clinical symptoms of COVID-19 (
12). We observed a triple vitamin deficiency that was significantly more prevalent among ICU patients. Interestingly, there was no vitamin E deficiency detected in the control group.
Vitamins and minerals have demonstrated their association with the proper functioning of the immune system, and their vital and often synergistic effects have been well-established (
6). In our study, lower levels of antioxidant vitamins, particularly vitamin E, were proportionally linked to the severity of the disease. Meta-analyses have reported varying effects of vitamin E supplementation on inflammatory cytokines, which may be attributed to different methodologies and variables of the study (
11,
33). Some studies have shown an association between disease severity, higher viral spread, and cell damage in various tissues. Similarly, lower IgM levels have been observed in mildly ill patients, which could be attributed to lower viral loads (
34). Accordingly, a negative correlation has been shown with IgM with time since symptom onset (
35). Similarly, our results have indicated significant differences in IgM levels among the different studied groups despite all participants having a vaccination history. These observations may suggest a decline in immunity in these individuals within three months after receiving two vaccine doses.
Vaccination has proven to be a reliable strategy against infectious diseases and pandemics. A meta-analysis by Ao et al. provided strong evidence that vaccination can reduce the risk of reinfection to less than 50% compared to unvaccinated individuals, and this protection may last for up to 12 months (
36). The effectiveness of vaccines, along with the milder cases of COVID-19 caused by the Omicron variant compared to previous variants, could significantly reduce the disease burden (
37). A nationwide Danish study by Nielsen et al. demonstrated that vaccinated individuals had a significant level of protection against SARS-CoV-2 reinfection compared to unvaccinated individuals. Although waning immunity following vaccination was observed, particularly during the Omicron period, vaccine effectiveness persisted for up to 9 months (
38). In our study, the patient groups experienced reinfection with SARS-CoV-2 within 6 months post-vaccination. Considering the predominant circulation of the Omicron variant, one of the factors contributing to reduced vaccine effectiveness could be the type of vaccine administered. However, we did not observe significant differences between the AstraZeneca and Sinopharm vaccines in terms of mean anti-SARS-CoV-2 immunoglobulin levels or the effects of vitamins A, C, and D among the different studied groups.
The beneficial effects are observed regardless of the type of vaccine. There is strong evidence indicating that neutralizing antibodies offer protection against COVID-19 (
39). The practical evidence presented in this study suggests that both the immunity induced by anti-COVID-19 vaccines and natural immunity acquired after SARS-CoV-2 infection provide protection against SARS-CoV-2 infection. However, due to the limited number of samples, it is not possible to assert this with absolute certainty. Nevertheless, vaccine effectiveness studies involving various vaccines have demonstrated a wide range of protection against reinfection (
40). Wajnberg et al. proposed that immune protection could be predicted by assessing neutralizing antibodies (
41). Although their results are based on limited data, they suggested a similar decline in neutralizing antibodies for both vaccine-induced and naturally acquired immunity. We examined total IgG and IgM levels against SARS-CoV-2, which could be valuable due to the highly conserved non-RBD domains with nearly identical sequences among related coronaviruses (
42).
5.1. Conclusions
In conclusion, vitamins C, E, and D3 play a crucial role in regulating immune activity by supporting various functions of the innate and adaptive immune systems. Inadequate levels of these vitamins can result in immune system dysfunction. The trio of vitamins assessed in this study may serve as potential biomarkers for protection against, and the severity of the disease provided that further details regarding clinical features or the disease's temporal evolution support the findings presented here.









 and vitamin (ng/mL) levels among patients and healthy individuals. The mean of each bar is presented in the figures. Mean vitamin levels decreased inversely with the disease severity; B, The mean IgM levels were highest in the ICU group and lowest in the control group; conversely, the IgG levels were highest in the control group and lowest in ICU patients.")
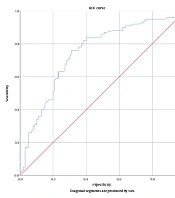
 analysis is used to identify the best biomarker among ICU and ward patients and determine the most effective biomarker among ICU and ward patients. IgG and IgG/IgM ratios served as excellent biomarkers, followed closely by Vit E levels, the Vit E/Vit C ratio (ratio EC), and Vit D levels. Additionally, the ratios of Vit D/Vit C (DC), Vit D/Vit E (DE), and IgG/IgM (IgGIgM) are also presented in the figure.")