


1. Background
Despite the progress in tuberculosis control programs and the development of strong anti-tuberculosis drugs and BCG vaccine, tuberculosis remains as one of the most important infectious diseases in the world with about 10 million morbidities and 1.3 million mortalities annually. To achieve the World Health Organization (WHO) agenda for ending tuberculosis by 2035, molecular genotyping of Mycobacterium tuberculosis can play an important role using different methods such as IS6110 RFLP, spoligotyping and especially mycobacterial-interspersed-repetitive-units (MIRU)-variable-number-of-tandem-repeats (VNTR) typing (1). For the diagnosis of tuberculosis, usually more than one clinical specimen is collected in different days and it is expected that M. tuberculosis genotypes are similar in all the samples. The determination of the genetic similarity of M. tuberculosis in a patient’s specimens can indicate the reproducibility of a method.
Reproducibility is a sign of precision of a measurement or test method. Some previous studies assessed the reproducibility of MIRU-VNTR. Supply et al. in the first paper published for the introduction of automated MIRU-VNTR method stated that 12-loci MIRU-VNTR typing was 100% reproducible, as all blinded duplicate samples analyzed were correctly assigned; they showed a small variation in the amplicon size of each locus in different repetitions (2). Gauthier et al. confirmed the repeatability and reproducibility of the automated MIRU-VNTR method (3). None of these studies assessed the MIRU-VNTR reproducibility among different M. tuberculosis isolates taken from the same patient on different days or different clinical samples. Since the diagnosis of tuberculosis usually is based on the preparation of several patient samples taken on different days, it provides a good opportunity to determine the reproducibility of the MIRU-VNTR method using different patient samples. In this study, the reproducibility was defined as the same MIRU-VNTR patterns among different isolates of a patient.
2. Objectives
The main objective of this study was to determine the reproducibility of 15-loci MIRU-VNTR method in different clinical samples isolated from confirmed patients.
3. Methods
During the study of M. tuberculosis genotyping by 15-loci MIRU-VNTR among tuberculosis patients in Golestan province, Southeast of Caspian Sea in Iran in 2016, we isolated 199 biochemically confirmed M. tuberculosis isolates from 162 tuberculosis patients (accepted for publication on 2019-07-28 in Iranian Red Crescent Medical Journal). There were 27 patients who had more than one culture-positive clinical sample. Out of 27 patients, 22 (81.48 %) had two confirmed M. tuberculosis isolates, four had three M. tuberculosis culture-positive isolates, and one patient had four confirmed M. tuberculosis isolates either from sputum or other clinical samples. Totally, 60 M. tuberculosis isolates were tested.
The DNA was extracted from the M. tuberculosis isolates by the boiling technique using 15 primers for MIRU-VNTR and PCR protocols has been used according to Gauthier et al. (3). The PCR product was detected by the 1.5% agarose gel electrophoresis and the copy number of each repeated allele was determined in comparison with the H37RV PCR product as the standard strain. The H37RV strain and distilled water were used as positive and negative controls of the MIRU-VNTR method, respectively (4). All tests were repeated two times unless a disagreement necessitated the third replication. The similarity of MIRU-VNTR panel for samples of each patient was evaluated using MIRU-VNTRplus online software available at http://www.miru-vntrplus.org.
4. Results
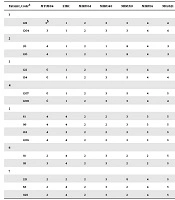
The 15-loci MIRU-VNTR patterns were similar in all samples of the same patient, giving the total number of 43 (71.67%) M. tuberculosis isolates belonging to 20 tuberculosis patients. Therefore, the reproducibility of about 71% was obtained. Mycobacterium tuberculosis isolated from seven other patients showed various levels of mismatch; in five patients (with 14 M. tuberculosis samples), the mismatch was found only on one locus or single locus variant (SLV) while a double locus variant (DLV) involving MTUB04 and MIRU31 was observed in two M. tuberculosis isolates from a single patient (Table 1). Based on the MIRU-VNTR plus database, the diagnosed M. tuberculosis genotypes were similar in all of these cases. Only one repeat of allelic differences was found in most cases with VNTR mismatch, except for isolates 26 and 136 for which the copy numbers of MIRU26 were two and seven, respectively (Table 1). In one case with three confirmed M. tuberculosis isolates, we found two exactly similar patterns belonging to new-1 genotype (codes 88 and 920 in Table 1) but another M. tuberculosis isolate (code 221) had different patterns related to the Delhi/CAS family.
| Patient, Codea | MTUB04 | ETRC | MIRU04 | MIRU40 | MIRU10 | MIRU16 | Mtub21 | QUB11B | ETRA | Mtub30 | MIRU26 | MIRU31 | Mtub39 | QUB26 | QUB4156 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | |||||||||||||||
| 128 | 3b | 1 | 2 | 3 | 3 | 4 | 4 | 3 | 4 | 4 | 5 | 4 | 3 | 8 | 4 |
| 1204 | 3 | 1 | 2 | 3 | 3 | 4 | 4 | 3 | 4 | 4 | 5 | 4 | 2 | 8 | 4 |
| 2 | |||||||||||||||
| 26 | 4 | 1 | 2 | 1 | 8 | 4 | 3 | 2 | 4 | 2 | 2 | 4 | 2 | 5 | 5 |
| 136 | 4 | 1 | 2 | 1 | 8 | 4 | 3 | 2 | 4 | 2 | 7 | 4 | 2 | 5 | 5 |
| 3 | |||||||||||||||
| 122 | 6 | 1 | 2 | 3 | 5 | 4 | 4 | 2 | 4 | 2 | 7 | 5 | 3 | 8 | 4 |
| 154 | 6 | 1 | 2 | 3 | 5 | 4 | 4 | 2 | 4 | 2 | 8 | 5 | 3 | 8 | 4 |
| 4 | |||||||||||||||
| 1207 | 6 | 1 | 2 | 3 | 5 | 4 | 5 | 2 | 4 | 2 | 7 | 6 | 3 | 8 | 5 |
| 1208 | 6 | 1 | 2 | 3 | 5 | 4 | 4 | 2 | 4 | 2 | 7 | 6 | 3 | 8 | 5 |
| 5 | |||||||||||||||
| 81 | 4 | 4 | 2 | 2 | 3 | 3 | 5 | 6 | 4 | 4 | 5 | 5 | 3 | 8 | 2 |
| 99 | 4 | 4 | 2 | 2 | 3 | 3 | 5 | 6 | 4 | 4 | 5 | 5 | 3 | 8 | 2 |
| 153 | 4 | 3 | 2 | 2 | 3 | 3 | 5 | 6 | 4 | 4 | 5 | 5 | 3 | 8 | 2 |
| 1205 | 4 | 4 | 2 | 2 | 3 | 3 | 5 | 6 | 4 | 4 | 5 | 5 | 3 | 8 | 2 |
| 6 | |||||||||||||||
| 91 | 2 | 4 | 2 | 3 | 2 | 2 | 5 | 2 | 3 | 2 | 5 | 3 | 3 | 7 | 2 |
| 93 | 3 | 4 | 2 | 3 | 2 | 2 | 5 | 2 | 3 | 2 | 5 | 2 | 3 | 7 | 2 |
| 7 | |||||||||||||||
| 221 | 2 | 2 | 2 | 3 | 6 | 4 | 5 | 2 | 3 | 2 | 8 | 4 | 3 | 8 | 2 |
| 88 | 2 | 4 | 2 | 3 | 2 | 4 | 5 | 2 | 3 | 2 | 2 | 3 | 3 | 7 | 2 |
| 920 | 2 | 4 | 2 | 3 | 2 | 4 | 5 | 2 | 3 | 2 | 2 | 3 | 3 | 7 | 2 |
aThe code number of patients.
bThe number of tandem repeats.
5. Discussion
MIRU-VNTR is a popular genotyping method for epidemiological purposes. Like any other laboratory test, high repeatability ensures that the results are reliable. In this study, the reproducibility was defined as the same 15-loci MIRU-VNTR patterns in different clinical samples of the same patient. We found that reproducibility was about 71% in our current study. In a few patients, different VNTR numbers were found only on one locus. Since the copy number of each locus in a PCR product was determined with the visualization of its product on the agarose gel, it seems that the mismatch may be due to in-house and manual method. The application of automated MIRU typing may reduce this defect and increase the reproducibility of the MIRU-VNTR method (5).
On the other hand, we found different genotypes in two samples of the same patient. In this case, it seems we faced a tuberculosis patient with mixed infections, which is not the subject of MIRU-VNTR reproducibility rejection. The presence of more than one genotype of M. tuberculosis in the same clinical sample (mixed or polyclonal infection) was defined in a previous study as the presence of more than one allele at one MIRU locus or more (6); however, in this study, the mixed infection was determined in different samples of the same patient collected on different days. It is not clear to us that this case was a true mixed infection or it occurred just because of the contamination of the sample with a new M. tuberculosis genotype; however, it would be very important if it was a true mixed infection.
Our results showed that out of 855 PCR processes that were done to determine the genotypes of 57 independent M. tuberculosis isolates (without isolates coded 88, 221, and 920) by the 15-loci MIRU-VNTR method, mismatch was observed only in 14 cases (1.64%); it means that the reproducibility of 15-loci MIRU-VNTR is more than 98% even with in-house PCR product detection. The reproducibility of a test or a technique can be measured by different methods such as inter-reader, operator-to-operator, lot-to-lot, and run-to-run reproducibility (7).
5.1. Conclusions
This is the first report of the reproducibility of a test based on the results of various samples from the same patient taken on different days. This sampling procedure is applicable for tuberculosis patients because more than one sample is needed to diagnose tuberculosis. This high reproducibility of MIRU-VNTR ensures that the results of this method are reliable.
