



1. Background
Multiple sclerosis (MS) is a chronic and degenerative disease of the central nervous system, which causes sensory disorders, malaise, muscle cramps, vision impairment, cognitive disorders, fatigue, tremor, urinary and excretory problems, sexual dysfunction, imbalance, amnesia, hearing loss, lethargy, blurry/double vision, and speech disorders (1, 2). MS often afflicts individuals of the productive age (3).
The complications of MS severely impact self-image and have debilitative effects on the adversity quotient (AQ) (4, 5). These complications increase the patients’ general stress on a daily basis, and their sense of shame and inferiority leads to inappropriate responses. When a stressful factor affects their lives, their cognitive activities become vulnerable, and behavioral problems emerge in the form of anxiety and depression, thereby decreasing the AQ. In addition to psychological complications and disorders, MS patients experience severe issues in their relationship with their spouse and children, which reduce their quality of life (QoL) and AQ (6). AQ is a major cognitive dimension, and its identification and enhancement create a hopeful attitude and improve the adaptability of patients when they are under psychological pressure (7).
MS patients suffer from emotional dysregulation and inability in cognitive emotion regulation (CER) due to the stresses caused by their disease (8). Emotionally competent individuals could improve their mental health status in the face of cognitive challenges (9). Patients occasionally suffer from emotional dysregulation due to the challenges of the disease, which threatens their emotional health and self-esteem (10). CER aims to support and form self-esteem and self-efficacy by increasing positive emotions and avoiding negative emotions in order to reinforce and form positive emotions. A high level of CER could restore the emotions of chronic patients (11).
It remains a matter of debate whether therapy could enhance the cognitive and emotional dimensions of MS patients. The choice theory (CT) effectively mitigates cognitive-emotional problems as it nurtures responsibility and creates a successful identity. In this therapy, the individual should identify the behavior they intend to modify and devote their attention to, while avoiding excuses for evading responsibility (12). The CT approach attempts to help the person identify their short-term and long-term goals, explicitly define these goals, evaluate ways of achieving these goals, choose a way that will lead to more desirable outcomes, and experience a more positive feeling toward themselves (13).
Behavioral activation (BA) is a therapeutic approach to the evaluation of patients’ behaviors (14, 15). In this therapy, the patient chooses alternative responses, performs the alternative responses, integrates these alternatives, and views and evaluates the outcomes (16). The goal of understanding in BA therapy is establishing a relationship between measures and emotional outcomes, as well as the systematic replacement of dysfunctional behavioral patterns with adaptive patterns. This therapy highlights social functioning quality and improvement. Overall, BA is a type of behavioral therapy that offers easily implemented and tangible techniques and is cost-effective owing to the short period of the treatment (17, 18).
Patients diagnosed with MS need adaptation and coordination with the challenges of their chronic disease since MS does not have a definitive cure (1). Guided imagery rescripting (ImRs) is assumed to affect adaptation to MS. Evidence suggests that the improvement rate of MS patients increases following guided ImRs (19). In the present study, BA therapy was integrated with guided ImRs; the latter encompasses mental exercises designed for the mental acceptance of health and improvement penetration into the body. In this approach, the visualization regions of the brain are activated, as when an experience is formed; in other words, the subject creates a stream of thought in which they could hear, sense, or express their desired feeling at the time and imagine the feeling. This therapeutic approach increases blood flow to the muscles and reduces fatigue in chronic patients (20).
2. Objectives
The present study aimed to determine the optimal therapeutic approach to improving the AQ and CER of MS patients.
3. Methods
3.1. Study Design
This quasi-experimental study was conducted with a pretest-posttest design and a control group.
3.2. Participants
The sample population of the study included the male and female MS patients visiting the Caspian Physiotherapy Center of Ahvaz, Iran in 2019. In total, 60 MS patients were selected via convenience sampling and randomly divided into three experimental groups (CT, BA therapy, and BA therapy with guided ImRs) and one control group (15 per each). In this study, 15 MS patients were allocated to each group using the G-power statistical software. The first experimental group received eight sessions of CT (90-minute weekly sessions), the second experimental group received eight sessions of BA therapy (90-minute weekly sessions), and the third experimental group received eight sessions of BA therapy with guided ImRs (90-minute weekly sessions). Tables 1-3 show a summary of the treatment sessions in the three experimental groups.
For ethical considerations, written informed consent was obtained from the participants prior to enrollment.
| Session | Details |
|---|---|
| 1 | Introducing the goals of the session; familiarizing the participants with the CT; laying out the rules of group counseling; expressing the goals of the sessions; explaining self and others’ evaluation; examining the goals, creating motivation, and encouraging the participants to partake actively |
| 2 | Familiarizing the participants with their identity; examining excuses for irresponsible behaviors; providing information about quality of life (QoL) improvement; encouraging the participants to discuss their current behavioral patterns |
| 3 | Familiarizing the participants with accepting responsibility for their behaviors; familiarizing the participants with the importance and necessity of responsibility in life |
| 4 | Familiarizing the participants with internal resistance based on the CT; relaxation skills training for mental health; carefully listening to the participants describing their feelings |
| 5 | Familiarizing the participants with their basic and effective needs in real life; explaining the effects of basic needs in life; assessing their ability to choose the best way to meet their basic needs; evaluating their level of commitment to the plan execution; discussing a sense of value and love as basic needs |
| 6 | Familiarizing the participants with planning for problem-solving; planning for their current life; behavioral evaluation; posing questions to challenge irrational thoughts |
| 7 | Familiarizing the participants with commitment to performance and the plan execution; examining responsibility for behavioral change; examining appropriate strategies for conflict resolution |
| 8 | Summarizing the exercises; resolving the problems faced in executing skills; explaining the necessity of using the skills in life for the management of stressful interpersonal situations; posttest |
| Session | Details |
|---|---|
| 1 | Pretest; establishing a therapeutic relationship with the patients; training on behavioral conventions |
| 2 | Training and focusing on behavior activation; person-environment interaction; training on proper strategies |
| 3 | Psychological training of therapeutic processes; behavioral conventions and revisiting behavioral systems |
| 4 | Focusing on disease stress and anxiety; using positive verbal reinforcement via hope therapy |
| 5 | Focusing on the patients’ cognitive-emotional dimensions; changing their mood and mental state |
| 6 | Focusing on and controlling behavioral states and judgments; revisiting behavioral judgments |
| 7 | Training on the medical, mental, and social components of the disease; training on coping skills; behavioral reconstruction |
| 8 | Presenting a summary of the therapy; survey; presenting the follow-up strategies; posttest |
| Session | Details |
|---|---|
| 1 | Pretest; establishing a therapeutic relationship with the patients; training on behavioral conventions; familiarizing the participants with ImRs; explaining the correlation between guided ImRs and thoughts |
| 2 | Training and focusing on behavioral activation; person-environment interaction; training on proper strategies; identifying irritating thoughts and images; identifying the correlation between thoughts, mental images, moods, emotions, and behaviors |
| 3 | Psychological training on therapeutic processes; behavioral conventions and revisiting behavioral systems; practicing muscle relaxation; imagining intrusive thoughts and images |
| 4 | Focusing on disease stress and anxiety; using positive verbal reinforcement through hope therapy; training on guided ImRs and guided imagery |
| 5 | Focusing on the patients’ cognitive-emotional dimensions; changing their mood and mental state; training on mental rotation and mental rehearsal |
| 6 | Focusing on and controlling behavioral states and judgments; revisiting behavioral judgments; practicing the cognitive reconstruction of negative thoughts and irritating images |
| 7 | Training on the medical, mental, and social components of the disease; training on coping skills; behavioral reconstruction; using the trained skills |
| 8 | Practicing and repeating the trained skills; survey; presenting the follow-up strategies; posttest |
3.3. Measures
3.3.1. Adversity Response Profile Questionnaire (ARPQ)
The Adversity Response Profile Questionnaire (ARPQ) was developed by Stoltz in 1997 to measure the AQ and provide an AQ profile. By presenting 14 situations, the questionnaire measures the reactions of the respondents to each situation through four questions, which are replicated for each situation. There are four situations for each general question, which are focused on control, ownership, reach, and endurance (CORE), respectively (total: 56 items). The items in the ARPQ are scored based on a five-point Likert scale (Completely Disagree = 1, Completely Agree = 5). Tamizi et al. (21) reported the Cronbach's alpha of 0.82 for the Persian version of the ARPQ, and the Cronbach's alpha coefficient was estimated at 0.88 for the entire questionnaire in the present study.
3.3.2. Cognitive Emotion Regulation Questionnaire (CERQ)
The Cognitive Emotion Regulation Questionnaire (CERQ) has been developed by Garnefski and Kraaij (22). It is a self-report measure with 36 items and two subscales of positive CER (putting into perspective, positive refocusing, positive reappraisal, acceptance, and refocus on planning) and negative CER (self-blame, other-blame, rumination, and catastrophizing). The items are scored from one (Almost Never) to five (Almost Always). In the CERQ, the positive and negative CER subscales consist of 20 and 16 items, respectively. Badie et al. (23) confirmed the reliability of the Persian version of the questionnaire at the Cronbach’s alpha coefficient of 0.88, and the Cronbach's alpha coefficient was estimated at 0.83 in the present study.
3.3.3. Demographic Information Questionnaire (DIQ)
In the present study, a researcher-made questionnaire was used to collect the demographic data of the participants, such as age, disease duration, and occupation status.
3.4. Statistical Analysis
Data analysis was performed in SPSS version 23.0 using descriptive and inferential statistics (e.g., mean and standard deviation), analysis of covariance (ANCOVA), and Bonferroni post-hoc test.
4. Results
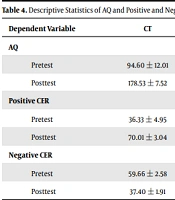
In total, 60 patients with MS with the mean age of 38.69 ± 6.78 years were enrolled in the study. The mean disease duration was 6.42 ± 2.38 years. Table 4 shows the mean values of the studied variables in the experimental and control groups at the pretest and posttest.
| Dependent Variable | CT | BA Therapy | BA Therapy with Guided ImRs | Control | P-Value |
|---|---|---|---|---|---|
| AQ | |||||
| Pretest | 94.60 ± 12.01 | 92.26 ± 10.19 | 93.77 ± 11.75 | 93.60 ± 22.25 | 0.723 |
| Posttest | 178.53 ± 7.52 | 181.60 ± 3.30 | 206.93 ± 5.57 | 92.54 ± 21.40 | 0.001 |
| Positive CER | |||||
| Pretest | 36.33 ± 4.95 | 27.39 ± 2.84 | 27.86 ± 2.72 | 28.33 ± 4.36 | 0.429 |
| Posttest | 70.01 ± 3.04 | 72.26 ± 2.74 | 87.66 ± 4.27 | 29.20 ± 4.45 | 0.001 |
| Negative CER | |||||
| Pretest | 59.66 ± 2.58 | 58.26 ± 3.09 | 58.93 ± 3.57 | 56.66 ± 4.70 | 0.372 |
| Posttest | 37.40 ± 1.91 | 35.43 ± 2.93 | 21.46 ± 3.70 | 55.86 ± 5.23 | 0.001 |
Abbreviations: AQ, adversity quotient; CER, cognitive emotion regulation; CT, choice theory; BA, behavioral activation.
aValues are expressed as mean ± standard deviation.
Based on the obtained results, the null hypothesis of the research was confirmed regarding the normal distribution of the scores of the control and three experimental groups in terms of the AQ, positive CER, and negative CER. However, the F-value for the interactive effects of the AQ, positive CER, and negative CER was not significant. Therefore, the regression homogeneity assumption was confirmed. Furthermore, the results of Levene's test for the AQ, positive CER, and negative CER were not significant. Therefore, the variances of the control and the three experimental groups were not considered significant for the AQ, positive CER, and negative CER. As a result, the variance homogeneity assumption was confirmed regarding the equality of the variances of the scores obtained by the patients in the control and experimental groups. By controlling the pretest, all the statistical tests were indicative of significant differences between the control and experimental groups in at least one dependent variable (F = 197.52; P < 0.001).
The findings showed significant differences between the CT and control groups in terms of the AQ (F = 748.38; P < 0.001), positive CER (F = 110.27; P < 0.001), and negative CER (F = 33.56; P < 0.001). Moreover, significant differences were denoted between the BA therapy and control groups in terms of the AQ (F = 1182.26; P < 0.001), positive CER (F = 82.20; P < 0.001), and negative CER (F = 38.12; P < 0.001). Significant differences were also observed between the BA therapy with guided ImRs and the control groups in terms of the AQ (F = 1061.06; P < 0.001), positive CER (F = 134.22; P < 0.001), and negative CER (F = 52.32; P < 0.001) (Table 5).
| Variables | SS | df | MS | F | P-Value | η2 | Power |
|---|---|---|---|---|---|---|---|
| CT | |||||||
| AQ | 10445.97 | 1 | 10445.97 | 748.38 | < 0.001 | 0.92 | 1.00 |
| Positive CER | 1545.66 | 1 | 1545.66 | 110.27 | < 0.001 | 0.84 | 1.00 |
| Negative CER | 477.86 | 1 | 477.86 | 33.56 | < 0.001 | 0.67 | 1.00 |
| BA therapy | |||||||
| AQ | 9927.69 | 1 | 9927.69 | 1182.26 | < 0.001 | 0.91 | 1.00 |
| Positive CER | 1300.31 | 1 | 1300.31 | 82.20 | < 0.001 | 0.83 | 1.00 |
| Negative CER | 613.92 | 1 | 613.92 | 38.12 | < 0.001 | 0.70 | 1.00 |
| BA therapy with guided ImRs | |||||||
| AQ | 16000.73 | 1 | 16000.73 | 1061.06 | < 0.001 | 0.98 | 1.00 |
| Positive CER | 2964.43 | 1 | 2964.43 | 134.22 | < 0.001 | 0.89 | 1.00 |
| Negative CER | 1251.90 | 1 | 1251.90 | 52.32 | < 0.001 | 0.76 | 1.00 |
Abbreviations: AQ, adversity quotient; CER, cognitive emotion regulation; CT, choice theory; BA, behavioral activation.
The mean difference (MD) of the CT and BA therapy was not considered significant for the AQ, positive CER, and negative CER. However, the MD of the CT and BA therapy with guided ImRs was considered significant for the AQ (MD = 26.62; P < 0.001), positive CER (MD = 16.59; P < 0.001), and negative CER (MD = 14.82; P < 0.001). In addition, the MD of the BA therapy and BA therapy with guided ImRs was significant for the AQ (MD = 29.44; P < 0.001), positive CER (MD = 15.20; P < 0.001), and negative CER (MD = 11.62; P < 0.001) (Table 6). Based on the mean values, BA with guided ImRs could enhance the AQ and positive CER of the MS patients and reduce their negative CER more significantly compared to the CT and BA therapy.
| Variables | Mean Difference | SE | P-Value |
|---|---|---|---|
| AQ | |||
| CT and BA therapy | 2.82 | 1.98 | 0.260 |
| CT and BA therapy with guided ImRs | 26.62 | 2.11 | < 0.001 |
| BA therapy and BA therapy with guided ImRs | 29.44 | 2.08 | < 0.001 |
| Positive CER | |||
| CT and BA therapy | 3.56 | 2.25 | 0.160 |
| CT and BA therapy with guided ImRs | 16.59 | 2.72 | < 0.001 |
| BA therapy and BA therapy with guided ImRs | 20.15 | 2.23 | < 0.001 |
| Negative CER | |||
| CT and BA therapy | 3.20 | 2.09 | 0.170 |
| CT and BA therapy with guided ImRs | 14.82 | 2.42 | < 0.001 |
| BA therapy and BA therapy with guided ImRs | 11.62 | 2.62 | < 0.001 |
Abbreviations: AQ, adversity quotient; CER, cognitive emotion regulation; CT, choice theory; BA, behavioral activation; SE, standard error.
5. Discussion
The present study aimed to investigate the effects of the CT and BA therapies with and without guided imagery rescripting on the AQ and cognitive emotion regulation of MS patients in Ahvaz, Iran. Significant differences were observed between the control and experimental groups in terms of the AQ, positive CER, and negative CER. The CT and BA therapy with and without guided ImRs could also increase the AQ and positive CER of the MS patients, while decreasing their negative CER. However, no significant differences were observed between the CT and BA therapy groups in terms of the other variables. Nevertheless, significant differences were denoted between the CT and BA therapy with guided ImRs and between BA therapies with and without guided ImRs in terms of the studied variables.
Based on the estimated mean values, BA therapy with guided ImRs could enhance the AQ and positive CER of the MS patients and reduce their negative CER more significantly compared to the CT and BA therapies. No similar studies had compared these three therapies; therefore, overlapping studies were examined in our research. For instance, Shahabi et al. (24) concluded that guided ImRs could effectively enhance positive emotion regulation and reduce negative emotion regulation in patients with cardiac disease. Furthermore, Vaziri et al. (25) reported that CT therapy could significantly increase a sense of responsibility in prisoners. Serrano-Ibanez et al. (26) also stated that BA therapy could significantly increase positive emotion regulation and reduce negative emotion regulation in patients with chronic musculoskeletal pain. The aforementioned findings are consistent with the results of the present study.
Perceiving psychological challenges and stressful conditions, MS patients experience low emotion regulation and AQ in the management of psychological challenges (27). Owing to the behavioral-motivational techniques of BA therapy, as well as mental exercises for mental acceptance, BA therapy integrated with guided ImRs could further improve the cognitive-emotional dimensions of MS patients. Compared to BA and CT therapies, the integrated form of these therapies has the advantage of mental preparation and imagination through integrating behavioral change based on a psychological model and self-care techniques with mental reconstruction (19). These advantages reinforce the AQ of chronic patients to manage psychological challenges and issues. With self-care based on motivation and goal imagination, this integrated therapy increased the acceptance of the MS patients toward the management of psychological stressors and challenges. Moreover, this therapeutic process enhanced the insight, thought control, and capacity of the MS patients for behavioral-emotional adaptation (28). In the current research, the intervention was based on the integration of two therapies, which resulted in the behavioral flexibility and thought change of the patients through altering their mental images. Ultimately, these techniques led to the mental acceptance, flexibility reconstruction, and higher emotional wellbeing of the MS patients by enhancing their AQ.
By integrating guided ImRs, selecting an alternative response, integrating the alternatives, viewing and evaluating the outcomes through mental exercises for mental acceptance, and integrating behavioral evaluation and mental exercises, the applied therapy in the present study could cultivate goal-orientation in acceptance, behavioral flexibility, and AQ (29). By increasing the blood flow to the muscles, reducing fatigue, and mental-behavioral relaxation, the integrated therapy enhanced the AQ of the MS patients in our research.
Using the behavioral change technique based on motivation and guided ImRs, which affects emotions, perceptions, thoughts, and behaviors (directly correlated with emotional problems), the integrated therapy used in the present study improved the emotion recognition, emotion evaluation, emotion expression, positive emotion evaluation, and use of emotional states to facilitate problem-solving (25). Furthermore, it could improve intelligent emotion regulation, the fight or flight response, reasonable emotion control, emotion regulation through negative emotion adjustment, and pleasant emotion enhancement without suppression.
The present study was performed on the MS patients visiting the Caspian Physiotherapy Center of Ahvaz. Therefore, the generalization of the results to other communities should be with caution due to different cultural backgrounds. No prior studies have compared the same therapies in young MS patients, which limited the reporting of consistencies between the findings. The training sessions of the experimental groups were held online due to the COVID-19 pandemic, which also might have limited the research process considering the patients’ problems.
5.1. Conclusions
According to the results, BA therapy with ImRs was more effective in enhancing the AQ and positive CER of the MS patients and decreasing their negative CER. Furthermore, the integrated therapy could promote the AQ and positive CER more effectively, while also reducing the negative CER of the MS patients more significantly compared to the CT and BA therapies. We used an integrated approach based on the behavioral change technique relying on motivation and thought expression through images, which led to dominance over negative mental pressures in the MS patients experiencing disintegrated psychological, social, emotional, and physical dimensions to enhance their mental and physical health. Therefore, it could be inferred that an integrated therapy may be more effective in the improvement of the AQ and positive/negative CER in MS patients. Counseling and treatment centers are recommended to pay special attention to the effectiveness of integrated therapies given their more significant effects on improving the health status of MS patients. Moreover, training workshops should be implemented by health authorities to train therapists on integrated therapies so that fundamental measures could be taken toward improving the AQ and positive/negative CER of MS patients.
