



1. Introduction
Congenital diaphragmatic hernia is a congenital diaphragmatic defect occurring in 1 per 3000 live births worldwide (1). It is fatal in 35% of infants, and the rest suffer chronic diseases such as reduced respiratory function and asthma (2). Moreover, the defect in the diaphragm allows abdominal viscera to protrude into the chest, causing mass effect and thereby preventing the natural development of the lung (3). Hernia through the subcostosternal part of the diaphragm that contains the omentum and intestine was first reported by an Italian anatomist in 1761 (4). In congenital diaphragmatic hernia, the defect may occur in the right, left or, in rare cases, both sides. This occurs contrary to the usual state in atypical cases, and the defect is manifested on the right and with the presence of the liver in the thoracic cavity (5). Different types of congenital diaphragmatic hernia include hiatus, Morgagni, and Bochdalek hernia. Bochdalek hernia is the most prevalent type of congenital hernia in which abdominal viscera enter the thoracic cavity due to a defect in the diaphragm, reducing the space for the development of the lung. As a result of pulmonary hypoplasia, many infants suffer from severe respiratory dysfunction immediately after birth, resuscitation, and operation. Esophageal hiatal hernias often demonstrate the signs of gastroesophageal reflux disease (GERD). The Morgagni hernia is rare, often diagnosed accidentally in regular ultrasound of asymptomatic patients (6). Any disorder in the fusion or musculinization of the anterior pleuroperitoneal membrane leads to an anatomic defect of the costosternal trigone, known as the Morgagni’s foramen. As the peritoneum is intact, Morgagni hernia has a true sac and, in most cases, the hernia sac only contains the omentum. However, the presence of the colon and, in rare cases, the small intestine and stomach has also been reported (7). Morgagni hernia is rare in the general population, and therefore few studies have been conducted on it (8). In children, Morgagni hernia may be associated with non-specific signs and confusing paraclinical presentation. Therefore, timely diagnostic and therapeutic measures can save the patient from death and severe complications (9).
2. Case Presentation
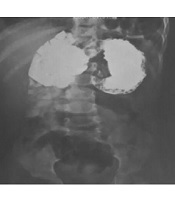
The patient was a one-year-old boy residing in the city of Kermanshah, Iran, visiting the hospital following cold signs one month before. After lung auscultation by the physician and performing chest radiography, the patient was referred to a pediatrician due to reduced lung sounds on the left side. The patient did not have dyspnea or a history of taking any specific medications. He had a history of physiological jaundice, and a hemangioma was found on the right eyelid in the examination of the face. After examining the patient’s state, he was hospitalized in Dr. Mohammad Kermanshahi Hospital. Cardiac consultation and echocardiography were performed, suggesting mild heart murmur, moderate ASD, VSD, mild shunt, and PS. In the chest radiography, the segments of the intestine and stomach were shown to have entered the left side of the thoracic cavity, and the heart and mediastinum were shifted to the right. Congenital diaphragmatic hernia in the left and the possibility of adenomatoid malformation of the left lung were reported for the patient. Furthermore, upper GI series showed part of the colon (spleen flexure) had entered the thorax, suggesting CDH diagnosis. The right lung was satisfactory. In the small intestine transit, part of the stomach fundus was observed in the lower half of the left side of thoracic cavity, suggesting sliding hiatal hernia. In the lower half of the left hemithorax, shadows were seen which were reported to be related to the sliding hiatal hernia (Figure 1).

Radiography before surgery. A, small intestine transit before the operation; B, radiography of the patient before the operation
3. Discussion
Morgagni hernia is a congenital defect of the diaphragm presenting with different signs, and its timely diagnosis and treatment are essential for the infant’s survival. In the present study, the initial signs were those of a common cold. However, careful examination revealed that the segments of the intestine and stomach had entered the left side of the thoracic cavity, and the heart and mediastinum were shifted to the right. Moreover, part of the colon had entered the thorax, and part of the stomach fundus was seen in the lower half of the left side of the thoracic cavity in the small intestine transit. Other studies have reported the entrance of colon to the thorax, and the small intestine transit. Congenital heart diseases are observed with Morgagni hernia in 58% of cases (10). However, according to some articles, this hernia may be asymptomatic and only present itself as a lesion on the stomach (9). Various surgical methods are available for repairing the hernial sac and returning the viscera to the abdomen. In the present study, open surgery through the abdomen like that used by Morgagni was selected (11). However, open surgery through the thorax, laparoscopy, and patch repair have also been reported for these patients (12-14). The patient underwent laparotomic surgery with left subcostal incision. After opening the site of the operation, findings suggested atypical Morgagni hernia. Contrary to the usual case, the defect continued to lateral and posterior parts as well. The colon, part of the stomach, and liver which were inside the left hemithorax were returned to the abdomen, the hernial defect was repaired (Figure 2), and the abdominal layers were repaired respectively.

During the surgery
3.1. Conclusions
Intraoperative findings suggested atypical Morgagni hernia. Therefore, it is recommended that physicians take into account rare types of hernia in their diagnoses, and perform more careful pre-operative radiography to be fully prepared. Clinical signs and findings during the patient follow-up suggested an improvement in his status and the repair of the defect caused by hernia (Figure 3).

Follow-up radiography
