



1. Background
Anterior cruciate ligament (ACL) reconstruction is a widely performed surgical procedure to restore knee stability in athletes following severe ligament injury. Over the years, ACL reconstruction techniques have evolved significantly, with various approaches developed to enhance knee stability and reduce postoperative complications. Among these, single-bundle and double-bundle ACL reconstruction techniques have been extensively studied, with findings indicating comparable long-term functional outcomes. However, the double-bundle technique sometimes provides superior rotational stability (1). Additionally, the all-inside ACL reconstruction technique, which minimizes bone removal and postoperative pain, has gained attention as a promising alternative, although it requires advanced surgical expertise (2). Moreover, improvements in graft fixation methods, such as bioabsorbable screws and suspensory fixation systems, have enhanced biomechanical stability while reducing the complications associated with traditional metal interference screws, including MRI distortion and implant removal requirements (3). Despite these advancements, rehabilitation following ACL reconstruction remains a significant challenge, particularly for athletes who engage in high-impact sports like volleyball. This underscores the need for further research to optimize recovery strategies and improve functional outcomes post-surgery.
The ACL injuries are common and costly in volleyball, with most occurring during non-contact landings, especially after spikes or blocks (4-6). Improper landing mechanics contribute significantly, as 84.6% of injuries happen during landing, with 76.9% following a spike (7). The financial burden is high, with surgery and rehabilitation costs reaching up to $30,000 per athlete, while over 50% fail to return to pre-injury performance levels (8). Prevention programs focusing on neuromuscular training (NMT), balance exercises, and proper landing techniques are essential to reduce these risks (5).
Reactive neuromuscular training (RNMT) challenges the neuromuscular system to respond quickly and efficiently to unexpected movements using tools such as balance balls, resistance bands, and medicine balls (9, 10). This method aims to improve stability, coordination, and proprioception (11), making it particularly relevant for athletes recovering from ACL injuries, including volleyball players, who require high levels of neuromuscular control for sport-specific activities such as jumping, landing, and rapid directional changes. The RNMT’s focus on enhancing static and dynamic balance, as supported by numerous studies (12-16), directly addresses the deficits commonly seen after ACL surgery and improves functional performance measures such as jump height, sprint speed, and agility (17-19). The rationale for selecting RNMT lies in its ability to mimic volleyball's unpredictable and dynamic nature, helping athletes regain sport-specific skills essential for a safe and effective return to play. Working with a qualified trainer ensures the safe implementation of exercises tailored to the athlete’s recovery needs (20).
Despite the growing interest in applying RNMT in rehabilitation, limited research addresses its specific effects on volleyball players with ACL reconstruction. Key gaps remain in understanding how RNMT impacts volleyball-specific performance metrics such as balance during dynamic movements, vertical jump height, agility, and reaction time, which are essential for effective gameplay. Additionally, the long-term sustainability of these improvements and their role in reducing the risk of re-injury have not been thoroughly examined. There is also a lack of comparative studies between RNMT and other sport-specific rehabilitation methods and limited investigation into its influence on psychological readiness and biomechanical adjustments in volleyball-specific actions like spiking and blocking.
2. Objectives
This study seeks to evaluate the effect of six weeks of RNMT on balance and performance in volleyball players with ACL reconstruction, aiming to establish its potential as an effective rehabilitation strategy tailored to the sport's unique demands.
3. Methods
3.1. Subjects
The present study was randomized trial research. The statistical population included male volleyball players in Quchan cty in 2022 - 2023 who had a history of ACL reconstruction surgery. The sample size was calculated using G*Power software (effect size = 0.5, alpha = 0.05, power = 0.95), resulting in 34 individuals for a t-test. Thirty male volleyball players with a history of ACL reconstruction in Quchan were selected based on inclusion and exclusion criteria. Participants were randomly assigned to two groups (exercise group: n = 15, control group: n = 15) using a simple random sampling method. Each participant received a unique number; a random number generator ensured unbiased allocation. Before participation, informed consent was obtained, and medical and sports history was recorded through questionnaires and interviews.
3.1.1. Inclusion Criteria
Age between 18 and 30 years (21); history of ACL reconstruction at least 12 months before the study commencement (22); return to sports participation with no reported limitations (4); at least three years of regular volleyball participation (23); average of 3 volleyball sessions per week; no history of persistent lower limb injuries (e.g., degenerative joint changes in the knee, unstable ankle, etc.); no significant lower limb abnormalities (hip anteversion, genu valgum, genu varum, tibial rotation, and flat feet); not currently participating in any ACL injury prevention training programs.
3.1.2. Exclusion Criteria
Inclouding: Non-compliance with study procedures (24); failure to complete the protocol; occurrence of a sports injury resulting in absence from training; development of pain during training; failure to complete the post-test (25); missing more than two training sessions.
3.2. Apparatus and Task
3.2.1. Y-Balance Test
The Y-Balance Test is a validated measure of dynamic balance (26) and assesses reach distance in three directions: Anterior, posteromedial, and posterolateral, arranged in a Y-configuration (135°, 135°, and 90°, respectively). The individual stands with their dominant foot at the center of the platform and extends the other foot to push the movable platform as far as possible without error before returning to a normal stance. The reach distance is measured from the movable platform to the center, averaged over three trials, normalized to leg length, and expressed as a percentage. The composite score is obtained by summing the three percentages and dividing by three (27). The test demonstrates high reliability, with intra-tester coefficients ranging from 0.85 to 0.91 and inter-tester reliability reaching 0.99 (27).
3.2.2. Vertical Jump Test
This test measures explosive lower extremity power in the vertical direction. The participant stands with feet shoulder-width apart and weight evenly distributed. They first mark the highest reachable point with a plastered finger (zero point), then jump as high as possible to mark the highest attainable point. The difference between these two points represents their performance. The test is repeated three times, and the average score is recorded (28).
3.2.3. Triple Hop Test
This test assesses the lower limb's power, speed, balance, and coordination over a specific distance. The participant stands with their dominant foot behind the starting line and performs three consecutive maximal jumps in a straight line using the same foot. The score is measured from the starting line to where the heel contacts the ground after the third jump. During the jumps, the hands remain stationary on the thighs. The test is performed thrice with the dominant foot, and the average score is recorded (29). Hamilton reported its reliability coefficient as 0.98 (30).
3.2.4. Single-Leg 6-Meter Timed Hop Test
This test evaluates the unilateral lower limb's power, speed, balance, and coordination over a set distance, focusing on time. A six-meter path is marked with designated start and finish points. The participant stands behind the starting line with hands behind them back to minimize upper body influence. At maximal speed, they perform consecutive hops along the path to cross the finish line. The total time from start to finish is recorded. The test is performed three times with the dominant foot, and the best time is considered the final score (28). Reliability coefficients range from 0.82 to 0.92 (28, 30).
3.3. Procedure
3.3.1. Reactive Neuromuscular Training Protocol
Pre- and post-intervention balance and performance assessments were conducted, including the Y-Balance Test, vertical jump test, triple hop test, and single-leg 6-meter timed hop test for all participants. After a 10-minute warm-up and familiarization with the tests, all subjects performed three valid trials of each test. After six weeks of the training protocol for the experimental group and daily life for the control group, all subjects participated in the post-test.
The RNMT protocol was designed to improve movement patterns through active participant involvement in error detection and enhanced feedback (10). Minimal verbal cues were provided to correct improper movement patterns, allowing participants to self-adjust. The program consisted of 18 sessions over six weeks, held three times a week, each lasting approximately 60 minutes under the supervision of an athletic trainer. Each session began with a 10-minute warm-up, followed by 40 minutes of RNMT exercises to improve balance, agility, and proprioception. Perturbation forces were applied using Thera-bands to challenge participants' stability. Exercise intensity was tailored individually using the Borg Scale, with the level maintained at or below 6 to prevent fatigue. The trainer closely monitored participants' movements, reducing improper knee valgus patterns and ensuring correct exercise execution.
The exercises included static and dynamic movements designed to engage target muscles. Exercises included maintaining balance with perturbation from Thera-bands, agility drills involving quick direction changes, and proprioceptive tasks to minimize abnormal joint movements. The control group continued their daily activities without any specific training, and changes in their routines were documented. The Borg Scale was chosen for its practicality and efficiency in assessing perceived exertion, making it ideal for this protocol's focus on controlled and moderate-intensity exercises (31). Heart rate or other intensity metrics were not employed, as the emphasis was on refining movement quality rather than cardiovascular endurance.
3.4. Data Analysis
Paired t-tests were used to evaluate changes in outcome measures pre- and post-intervention within each group. Additionally, analysis of covariance (ANCOVA) was conducted to compare outcomes between the intervention and control groups. All analyses were performed using SPSS version 22, with a significance level set at P ≤ 0.05.
4. Results
The statistical indices of age, height, and weight of the participants in experimental and control groups are shown in (Table 1).
| Variables | Number | Mean ± SD | P-Value |
|---|---|---|---|
| Age | 0.0003 | ||
| Experimental | 15 | 25.86 ± 3.35 | |
| Control | 15 | 23.06 ± 3.67 | |
| Height | 0.582 | ||
| Experimental | 15 | 177.53 ± 5.69 | |
| Control | 15 | 178.80 ± 7.02 | |
| Weight | 0.568 | ||
| Experimental | 15 | 71.73 ± 5.81 | |
| Control | 15 | 69.86 ± 5.20 |
Statistical Indices Related to the Participant’s Age, Height, and Weight
The Shapiro-Wilk test confirmed the normality of the distribution of research variables data at both the experimental stages and among the experimental groups (P > 0.05). Levene's test (P > 0.05) examined the assumption of equality of variances, and the homogeneity of variances between the groups was confirmed. Additionally, the results of the homogeneity of regression slope test indicated that the homogeneity of regression slope was satisfied.
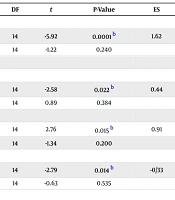
The impact of the intervention on balance and performance was evaluated using a dependent t-test from the pre-test to the post-test. The results showed that the intervention significantly improved balance, triple hop test, single-leg 6-meter timed hop test, and vertical jump height in the experimental group. No significant improvements were observed in the control group for any variables (Table 2).
| Variables | Pre-test | Post-test | df | t | P-Value | ES |
|---|---|---|---|---|---|---|
| Balance | 1.62 | |||||
| E | 96.46 ± 1.15 | 98.86 ± 1.74 | 14 | -5.92 | 0.0001 b | |
| C | 97.04 ± 0.97 | 97.51 ± 1.14 | 14 | -1.22 | 0.240 | |
| Performance | ||||||
| TH test | 0.44 | |||||
| E | 414.53 ± 29.42 | 439.26 ± 24.19 | 14 | -2.58 | 0.022 b | |
| C | 423.33 ± 35.05 | 411.33 ± 36.88 | 14 | 0.89 | 0.384 | |
| Sl-6MTH test | 0.91 | |||||
| E | 3.08 ± 0.24 | 2.79 ± 0.29 | 14 | 2.76 | 0.015 b | |
| C | 2.97 ± 0.27 | 3.05 ± 0.22 | 14 | -1.34 | 0.200 | |
| VJH test | -0.33 | |||||
| E | 39.66 ± 3.49 | 44.13 ± 4.58 | 14 | -2.79 | 0.014 b | |
| C | 39.40 ± 3.08 | 40.20 ± 3.36 | 14 | -0.63 | 0.535 |
The Results of the Dependent t-Test for Intragroup Comparison of the Balance Variable a
For between-group comparisons, an ANCOVA was used. The results showed a significant difference between the experimental and control groups in balance and all performance components. This means that after controlling for the pre-test effect, there was a significant difference in balance, triple hop test, single-leg 6-meter timed hop test, and vertical jump between the control and experimental groups. The results indicate that the means of that measure were significantly higher in volleyball players with ACL injuries compared to the control group (Table 3).
| Variables and Groups | Pre-test | Post-test | SS | df | MS | F | P-Value | ES |
|---|---|---|---|---|---|---|---|---|
| Balance | - | - | - | - | - | - | ||
| E | 96.46 ± 1.15 | 98.86 ± 1.74 | ||||||
| C | 97.04 ± 0.97 | 97.51 ± 1.14 | ||||||
| Performance | ||||||||
| TH test | 5728.67 | 1 | 5728.67 | 5.67 | 0.024 | 0.174 | ||
| E | 414.53 ± 29.42 | 439.26 ± 24.19 | ||||||
| C | 423.33 ± 35.05 | 411.33 ± 36.88 | ||||||
| SL-6MTH test | 0.57 | 1 | 0.57 | 8.24 | 0.008 | 0.234 | ||
| E | 3.08 ± 0.24 | 2.79 ± 0.29 | ||||||
| C | 2.97 ± 0.27 | 3.05 ± 0.22 | ||||||
| VJH test | 118.76 | 1 | 118.76 | 7.26 | 0.012 | 0.212 | ||
| E | 39.66 ± 3.49 | 44.13 ± 4.58 | ||||||
| C | 39.40 ± 3.08 | 40.20 ± 3.36 |
The Results of the Analysis of Covariance Test to Compare the Exercise Groups in the Variables of Balance and Performance a
5. Discussion
The study aimed to investigate the impact of six weeks of RNMT on balance and performance in volleyball players with ACL injuries. The results indicated significant improvements in balance, as measured by the Y Balance Test, and performance, as measured by the Vertical Jump Test, triple hop test, and Single-Leg 6m Timed Hop Test, in the intervention group compared to the control group. These findings suggest that RNMT may be an effective intervention for improving balance and performance in volleyball players recovering from ACL reconstruction.
The results showed that RNMT training significantly improved dynamic balance in volleyball players with reconstructed ACLs. These findings align with recently studies (13-16, 32-34). Like Guzmán-Muñoz et al. (13), who reported improved balance and functional performance in individuals with functional ankle instability after neuromuscular interventions, this study highlights the adaptability of NMT across different injury types. Additionally, the findings are consistent with Saki et al. (15), who demonstrated significant balance and performance gains following core stability exercises, reinforcing the effectiveness of neuromuscular interventions. However, differences in statistical methods (ANCOVA vs. repeated ANOVA) and measured outcomes (e.g., Saki’s focus on dynamic balance vs. this study’s emphasis on vertical jump height and hop tests) highlight variations in research design and priorities (15).
Khalid et al. (14) reported significant NMT benefits in ACL rehabilitation, including improved hop performance, pain reduction, and enhanced Cincinnati knee scores. While this study did not assess pain or quality of life, both studies highlight NMT’s role in restoring function and optimizing athletic performance. Similarly, Sikora et al. (34) found improvements in dynamic balance and jump performance following NMT. However, they also assessed the Reactive Strength Index (RSI) and landing biomechanics, reflecting different sport-specific demands. Mirzaee et al. (33) emphasized joint position sense (JPS) and dynamic balance improvements in athletes with knee valgus, further supporting the proprioceptive benefits of NMT. Belamjahad et al. (32) also found NMT beneficial for jump height and balance. However, they focused on sprint and change-of-direction speed, which were not examined in this study, highlighting sport-specific adaptations in soccer versus volleyball.
Contrastingly, Yadollahi et al. (16) focused on landing kinematics, particularly hip flexion angles, in basketball players and did not observe significant improvements in balance. While the kinematic outcomes were not measured in the current study, both investigations demonstrate improvements in functional performance, albeit with different focal points. This contrast highlights how intervention goals influence outcome selection and interpretation.
The results demonstrated that RNMT significantly improved volleyball players' performance in the triple hop test, single-leg 6-meter timed hop test, and vertical jump height, which are crucial for functional recovery after ACL reconstruction. These findings align with previous studies on RNMT's impact on performance in individuals with musculoskeletal injuries (17, 19). Mohammadi et al. (17) found that corrective exercises in basketball players with dynamic knee valgus significantly improved knee joint strength, range of motion, and performance, contributing to injury prevention. Similarly, Rajasekar et al. (19) reported that kinesio taping effectively reduced dynamic knee valgus in both men and women immediately after application. Enhanced performance can help athletes return to sports more safely and efficiently while improving their overall quality of life. Additionally, the significant difference between the experimental and control groups suggests that the observed improvements in balance and performance were likely due to RNMT training.
The RNMT is a specialized training method to improve neuromuscular control, proprioception, and reaction time. Incorporating balance and coordination exercises enhances knee joint stability, reduces re-injury risk, and boosts athletic performance. The findings of this study align with previous research, demonstrating RNMT’s effectiveness in enhancing neuromuscular control, proprioception, and lower extremity strength, facilitating a faster return to sport while minimizing re-injury risks. However, limitations such as a small sample size, short intervention duration, and lack of gender-specific analysis may affect the generalizability of the results. Despite these constraints, the study highlights the potential of RNMT in improving balance and performance, which are essential for volleyball players recovering from ACL reconstruction to safely and effectively resume high-impact activities.
Clinically, the findings of this study have important implications for the rehabilitation of volleyball players with ACL injuries. The results suggest that incorporating RNMT into rehabilitation programs may enhance functional outcomes and facilitate a safe return to sport. Future research with larger samples, a longer follow-up period, and an examination of gender-specific effects is warranted. Furthermore, future studies should explore the impact of RNMT on other performance parameters, such as agility, speed, and muscle strength, to provide a more comprehensive understanding of its effects in this population. In conclusion, this study supports using RNMT as an effective intervention for improving balance and performance in volleyball players with ACL injuries. The findings have important implications for clinical practice and highlight the need for further research to optimize the use of this training modality for this population.
