


1. Background
Coronary artery disease (CAD) is the most common reason for death all over the world (1). Coronary artery disease accounts for 50% of annual deaths and 79% of death from chronic conditions in Iran (2). Coronary artery disease may be classified as stable angina (SA), unstable angina (UA), non-ST elevation myocardial infarction (NSTEMI), and finally, ST elevation myocardial infarction (STEMI). Various therapeutic interventions are adopted to prevent myocardial damage based on the patient's clinical condition (3). Although time is a major factor in infarct size development, a critical approach, including prompt diagnosis and early management, should be made in STEMI patients (4). Nowadays, primary percutaneous coronary intervention (PPCI) has remained the main dominant reperfusion therapy for STEMI (5).
Studies often focus on assessing PPCI-related outcomes such as mortality and major adverse events. But, few studies have been conducted to assess the psychological aspect, including quality of life (QOL) (6). Quality of life is an important outcome after PPCI and is defined as an individual's perception of their position in life based on the cultural and social context considering their goals, hopes, standards, and personality (7). A study in Jakarta showed the score of QOL was 68.36 (21.24) in post-PPCI patients (8). Another study conducted three years after PPCI in STEMI patients revealed a low physical component score was associated with a high prevalence of hypertension (9).
Cognitive behavioral therapy (CBT) is a non-pharmacological therapy guided by an experimental orientation to human behavior (10). An RCT conducted on heart failure patients showed that 12 weeks of CBT intervention improved their quality of life (11). Another RCT on cardiac surgery patients revealed positive effects of 9-month-CBT heart rate variability quality of life (12).
2. Objectives
Given that PPCI patients experience the sudden event of cardiac intervention, they may be unable to adapt to the situation. Also, the literature review showed that their quality of life might be affected post-PPCI. So, the present study aimed to determine the effect of CBT on quality of life in patients with CAD.
3. Methods
This randomized experimental study was conducted on 30 CAD patients who underwent primary percutaneous coronary intervention (PPCI) in a cardiac clinic affiliated with Mazandaran University of Medical Science, Iran (15 patients in each group).
The participants were selected using a convenience sampling method based on inclusion criteria. Then, they were randomly allocated to two groups using a computer-generated random number system. The sample size was calculated based on previous studies. During the study, none of the patients were excluded. The intervention was conducted on scheduled separate days of the week to prevent interaction between the two groups.
The inclusion criteria were all CAD patients who underwent PPCI, were 30 to 60 years old, willing to participate, had minimum literacy, and did not have physical and psychological disorders (including blinding, psychosis, etc.). Patients unwilling to continue cooperation, hospitalization, and death were excluded.
The data collection tools included demographic information on age, gender, etc. The next tool was the short form-36 health survey (SF-36). The questionnaire was designed by Ware et al. to assess the quality of life and consists of 36 items with two general performance measures, including the physical component summary (PCS) and the mental component summary (MCS). This scale also consists of eight health constructs: Physical functioning (10 items), physical role functioning (four items), bodily pain (two items), the general perception of health (five items), energy and vitality (four items), social functioning (two items), emotional role functioning (three items) and mental health (five items). The total range of scores is 0 - 100. The overall score includes two categories, physical and mental. A higher score on the scale for each domain indicates a better quality of life (13, 14). The reliability of this questionnaire was conducted on the Iranian population via Cronbach's Alpha. It was 0.91 and 0.87 for PCS and MCS, respectively (15). In the present population, the reliability via Cronbach's alpha was 0.88 for overall SF-36.
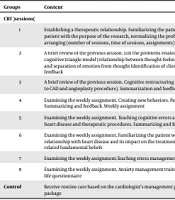
After obtaining written permission from the Ethics Committee of Islamic Azad University, Gorgan branch, the researcher introduced himself to the patients, and then he explained the procedures of the study to them. The intervention was performed in eight consecutively sessions. The eligible patients completed demographic data and SF-36 quality of life in the first intervention session. The content of the sessions is provided in Table 1. Forty-five days after the last session, a posttest of SF-36 quality of life was completed in each group.
| Groups | Content |
|---|---|
| CBT (sessions) | |
| 1 | Establishing a therapeutic relationship. Familiarizing the patient with CAD (causes, including the psychological causes of CAD). Familiarizing the patient with the purpose of the research, normalizing the problem and creating hope, checking the patient's expectations from the treatment, arranging (number of sessions, time of sessions, assignments) |
| 2 | A brief review of the previous session. List the problems related to CAD. Classification of the problems with the help of the patient. Training the cognitive triangle model (relationship between thought-feeling-behavior and the difference between them) Training and recognition of the emotion and separation of emotion from thought Identification of client's emotions and scoring based on the intensity of emotion. Summarization and feedback |
| 3 | A brief review of the previous session. Cognitive restructuring (identification, evaluation, change, and correction of self-occurring thoughts related to CAD and angioplasty procedure). Summarization and feedback. Presentation of the weekly assignment worksheet |
| 4 | Examining the weekly assignment. Creating new behaviors. Paying attention to the behavioral chain (related to CAD and angioplasty procedure). Summarizing and feedback. Weekly assignment |
| 5 | Examining the weekly assignment. Teaching cognitive errors and inefficient thinking. Examining the cognitive errors of clients in connection with heart disease and therapeutic procedures. Summarizing and feedback. Presentation of cognitive errors identification worksheet. |
| 6 | Examining the weekly assignment. Familiarizing the patient with the fundamental beliefs related to CAD Identifying the patient's attitudes and their relationship with heart disease and its impact on the treatment process and compliance with the treatment. Providing a worksheet to identify the related fundamental beliefs |
| 7 | Examining the weekly assignment.Teaching stress management, self-control, and raising mood |
| 8 | Examining the weekly assignment. Anxiety management training and ways to improve the quality of life. Completing the posttest (SP-36) quality of life questionnaire |
| Control | Receive routine care based on the cardiologist's management plan. After completing the intervention, CBT content provided in a psychological care package |
The present study was approved by the Ethics Committee of Islamic Azad University, Gorgan branch (IR.IAU.SARI.REC.1401.068). All the procedure was explained to participants, and signed informed written consent was obtained.
The data were analyzed using IBM SPSS version 24.0 (Statistical Package for the Social Sciences, Chicago, IL). Shapiro-Wilk test was applied to test the normality distribution. The frequency, mean, and standard deviation was used to describe the variables. The chi-square test was used to explore the independent nature of some categorical variables. The ANCOVA test made the comparison of the means between the two groups. A P-value less than 0.05 is considered statistically significant.
4. Results
The present study showed that most patients were at least 35 years old, male, married, BSc, living in the city, and had no previous disease history and surgery (Table 2). The chi-square test showed a non-significant difference between the two groups regarding demographic variables (P > 0.05).
| Variables | Groups | P-Value a | |
|---|---|---|---|
| CBT (N = 15) | Control (N = 15) | ||
| Age (y) | 0.598 | ||
| < 34 | 1 (6.6) | 3 (20.0) | |
| ≥ 35 | 14 (93.3) | 12 (80.0) | |
| Gender | 1.000 | ||
| Female | 5 (33.4) | 5 (33.4) | |
| Male | 10 (66.6) | 10 (66.6) | |
| Marital status | 1.000 | ||
| Single | 3 (20.0) | 4 (26.7) | |
| Married | 12 (80.0) | 11 (73.3) | |
| Educational level | 0.801 | ||
| Diploma | 9 (60.0) | 9 (60.0) | |
| BSc | 4 (26.6) | 5 (33.3) | |
| MSc | 2 (13.4) | 1 (6.6) | |
| Living place | 1.000 | ||
| City | 10 (66.6) | 9 (60.0) | |
| Village | 5 (33.4) | 6 (40.0) | |
| Disease history | 1.000 | ||
| No | 12 (80.0) | 12 (80.0) | |
| Yes | 3 (20.0) | 3 (20.0) | |
| Stent number | 1.000 | ||
| One | 10 (66.6) | 9 (60.0) | |
| Two | 5 (33.4) | 6 (40.0) | |
| Surgery history | 1.000 | ||
| Yes | 5 (33.4) | 5 (33.4) | |
| No | 10 (66.6) | 10 (66.6) | |
a Chi-square
A comparison of the mean (SD) of the QOL score before and after the CBT intervention is provided in Table 3. The results of the ANCOVA test showed that the mean quality of life score in the CBT group was significantly better than in the control group (P < 0.001, effect size = 0.650).
| QOL | Groups | F | P-Value a | Partial Ecta Squared | |
|---|---|---|---|---|---|
| CBT (Mean ± SD) | Control (Mean ± SD) | ||||
| Before intervention | 136.2 ± 5.0 | 134.8 ± 3.5 | 52.018 | < 0.001 | 0.650 |
| After intervention | 145.4 ± 7.0 | 130.0 ± 4.4 | |||
a ANCOVA
5. Discussion
The present experimental study aimed to determine the effect of CBT on the quality of life the CAD patients. The results showed that the QOL score significantly improved in the CBT group but significantly decreased in the control group. A systematic review study showed QOL was affected after cardiac surgery, so the patients expressed this challenge after cardiac surgery (16). An RCT in Iran on 56 cardiac patients showed that 8 sessions of CBT could improve the total score of the QOL (17). A study on cardiac patients revealed CBT positively affected anxiety as a risk factor for CAD that affects the QOL (18). As a multi-dimensional intervention, CBT can consider the psychological aspect of PPCI events, so it can be a helpful choice.
An RCT on chronic CAD patients showed that a 12-week CBT intervention could decrease their stress, depression, and anxiety (19). But another cross-sectional study showed angioplasty increased the mean score of QOL (20). The last study was performed to show the positive effect of this intervention as a medical choice in this regard. But ignoring the psychological aspect of the QOL of the patient.
The present RCT showed that an 8-session CBT intervention could improve the QOL score of PPCI patients. They experienced sudden events without a previous mentality that helped them to cope with changing conditions. The results also showed that the QOL score decreased if no intervention was performed. So, therapeutic intervention is necessary in this regard. CBT can be considered a non-pharmacological intervention that is necessary for PPCI patients.
The limitation of the present study was the small sample size and the mental status of the patients in CBT sessions that affected the results of the QOL score.
