



1. Background
Visual impairments are one of the public health problems that many people in the world suffer from due to the increase in the elderly population and various diseases (1). According to research, the most common and important cause of vision disorders is diabetes (2). In 2017, the International Diabetes Federation (IDF) estimated that 451 million people (aged 18 - 99 years) had diabetes worldwide, which is expected to increase to 693 million by 2045 (3). According to the latest statistics announced by the Iranian Diabetes Association, 7 million Iranians (8.9%) suffer from diabetes. This is although this statistic triples every 15 years (4). Also, according to statistical data, it is estimated that the global number of people suffering from DRVI will increase from 126.6 million in 2010 to 191 million people by 2030 (3). Unfortunately, our country has no accurate statistics on people with DRVI. In the study by Olfatifar et al., the prevalence of vision disorders caused by type 2 diabetes was reported as 47.55% (5), and in the study by Mahmoudi Nezhad et al., the highest prevalence of retinopathy was reported in the eye clinic at 57.8% (6).
If diabetes is not effectively controlled, it can lead to serious risks such as cardiovascular disease, shock, retinopathy, neuropathy, and nephropathy (7). This disease profoundly affects a person's mental, physical, and social health and causes disabilities (8). Due to the complex nature of the disease and its management, these patients pose special challenges for healthcare providers (9).
All recipients of services in health care centers have expectations of nurses and the health system based on the nature of the disease, socio-cultural context, and their previous experiences (10). Expectations are beliefs about future events (11). Nowadays, every client's right is to have access to high-quality services (12). The increasing prevalence of diabetes and its associated costs in the United States indicate that new strategies in healthcare delivery are needed to help better manage the disease and achieve better outcomes (13). Even with the advancement of medical science, patients with diabetic vision disorders are still seen in vision rehabilitation services. These patients have unique and complex needs, and understanding this difference helps professionals design their clinical practices by considering their expectations. Therefore, paying attention to the expectations of these patients and examining their consequences can be of particular importance (9).
The health system faces great challenges in meeting the needs and expectations of patients with low vision due to diabetes, considering their special cultural and social context (14). By knowing patients' expectations, health professionals can better meet reasonable demands (15). This issue is also emphasized in health policies. In terms of health policy, services must follow patients' wishes, needs, and preferences and be responsive to them (16, 17). In 2000, the World Health Organization (WHO) declared that one of the health system's main goals is to meet patients' expectations (18). Also, historically, the highest structural innovation in health care is the paradigm shift of health service systems toward patient-centeredness. Despite these facts, policymakers and healthcare professionals have paid little attention to patients' expectations and needs (14) and often ignore their patients' expectations and concerns, which can negatively affect the health dimension (15). A number of studies also show that some of the client's needs are unmet, and there are significant areas for improving the non-objective aspects of healthcare quality (11). Furthermore, studies have shown that most health staff do not know enough about the care programs for these patients; if the disease is properly controlled and appropriate education and care are provided per individual expectations, the development of DRVI can be prevented to some extent (19).
According to most studies, DRVI is considered normal by health professionals, and the provision of services, especially in developing countries, is only in the form of routine care, and the unique expectations and needs of these patients are not taken into account (19). While patient-centered care is essentially care based on patients' wishes, expectations, and preferences and seeks to fulfill them (20). Patient-centered care, as a key component of the health system, ensures the access of all patients to that special individual care (21). Donabedian stated that meeting the needs and expectations of clients should be the ultimate goal of the health system, and examining the level of achieving them should be the final evaluation of the outcome of health care and services (22).
Due to the importance of service quality in the health sector, a fundamental action for quality improvement programs can be to assess the expectations of service recipients regarding the quality and usefulness of the services provided (23) and examine the consequences of meeting the expectations of visually impaired patients with diabetes can provide an opportunity to identify weaknesses in services and to correct them in the future (12). Since in the present study, theories and research literature about the phenomenon under study were limited, to reach the goal of the present study, a qualitative study using the qualitative content analysis method was used; because among the qualitative research methods, this method was suitable for the nature of the present research in terms of providing an objective description and identifying the hidden and obvious categories of the message (24, 25). This method allows the researcher to obtain what exists and what patients have experienced without any presuppositions (26, 27).
2. Objectives
Considering the importance of patient expectations and the consequences of meeting them by healthcare service providers, the purpose of this study was to investigate the consequences of meeting the expectations of visually impaired patients caused by diabetes using a qualitative study.
3. Methods
3.1. Study Design
The present study's qualitative methodology helped gain in-depth insights into the consequences of meeting health expectations in patients with low vision due to diabetes. This article is reported according to COREQ guidelines.
3.2. Study Population and Sampling
Our study population was 13 people; 10 patients with DRVI, two nurses, and one member of the patient's family. In order to recruit participants at an ophthalmology teaching hospital from November 2020 to May 2021, purposeful sampling was used as the best sampling method in qualitative studies. This hospital was chosen due to the ease of access to samples. The inclusion criteria included diabetes, having ocular complications due to diabetes, visual acuity ≤ 5/10, no cognitive and psychological problems, and the ability to communicate. The exclusion criteria included the voluntary withdrawal of the patient from the study or the creation of unpredictable problems, such as illness or any problem that disrupts the continuation of the study. The selection of participants in this study was based on maximum diversity in terms of demographic characteristics. The first author (MA), previously trained in interviewing and communication techniques, conducted all interviews. Interviews were conducted individually, in depth, semi-structured, and face-to-face. Sampling continued until data saturation, and 13 participants were interviewed. Patients with low vision due to diabetes were interviewed twice and the rest once. A total of 23 interviews were conducted with 13 participants. The duration of the interviews was 35 to 55 min in the first round and 10 to 20 min in the second round.
3.3. Data Collection and Analysis
A short researcher-made questionnaire was used to collect the demographic and contact information of the participants. The interviews began with guiding questions (as a person with low vision due to diabetes, please express your experiences of having expectations and needs met by the health system), and then the interview continued with exploratory questions (Please explain what are the shortages of the services and care you receive from the health system compared to your condition? And what kind of service would you like to receive?). In this study, the conventional content analysis proposed by Graneheim and Lundman was used to analyze the data (25). Therefore, categories were extracted directly from the interview data without considering pre-defined categories. Microsoft Word 2016 and MAXQDA 2010 software were used to transcribe the interviews and manage and analyze the data.
In order to analyze the data, after each interview, the first author (MA) listened to the audio file, transcribed the interviews, and interpreted them verbatim. The full text of each interview was read several times to fully understand it. Sentences and paragraphs related to research questions and objectives were identified, inductively coded, compared based on similarities and differences, and finally classified into emerging categories and sub-categories. Codes and categories were reviewed with other authors, and a final consensus was reached.
3.4. Rigor
In this study, four criteria proposed by Lincoln et al. were used to increase the trustworthiness of the data (credibility, dependability, confirmability, and transferability) (28, 29). In this research, from cases such as Long-term interaction with the data, spending enough time to collect more in-depth data, selecting participants with maximum diversity, conducting interviews with the necessary patience and without prejudice, member checking, regular and accurate data collection, review by experts, preservation of research documents and accurate recording of all research stages (audio recording, text, notes, analysis), and full expression of the details of the study and the participants was used. The researcher also tried to ask all the participants questions in the same field and record all the interviews and write them down word by word.
3.5. Ethical Consideration
Before starting the study, the study's purpose and interview process were provided to the participants, and verbal and written informed consent was obtained for interviewing and recording them, emphasizing the confidentiality of the information. Voluntary withdrawal at any study stage was free at the participant's request. Also, the study protocol was approved by the Tehran University of Medical Sciences (TUMS) before data collection (approval ID: IR.TUMS.FNM.REC.1399/039).
4. Results
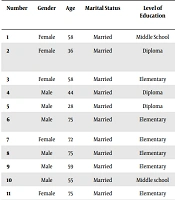
Participants in the present study included ten patients with DRVI, two nurses, and one member of the patient's family. The mean (standard deviation) age of the participants was 54.69 (16.63). One participant had type 1 diabetes, and nine had type 2 diabetes. The disease duration of the participants was 1 - 30 years. Five patients were hospitalized for cataracts, one for cataract and retinopathy, and four for retinopathy. Almost all participants, except one patient, had a history of previous hospitalization (Table 1).
| Number | Gender | Age | Marital Status | Level of Education | Job | Visual Acuity | Duration of Diabetes (y) | Duration of Visual Impairment (y) |
|---|---|---|---|---|---|---|---|---|
| 1 | Female | 58 | Married | Middle school | Housewife | OD: 1/10; OS: 4/10 | 15 | 5 |
| 2 | Female | 36 | Married | Diploma | Housewife, patients’ companion | - | - | - |
| 3 | Female | 58 | Married | Elementary | Housewife | OD: 4/10; OS: 1/10 | 12 | 4 |
| 4 | Male | 44 | Married | Diploma | Self-employment | OD: 3/10; OS: HM | 19 | 8.5 |
| 5 | Male | 28 | Married | Diploma | Employee | OD: 1m CF; OS: LP | 20 | 9.5 |
| 6 | Male | 75 | Married | Elementary | Self-employment | OD: 3.5m CF; OS: 1.5m CF | 7 | 3 |
| 7 | Female | 72 | Married | Elementary | Housewife | OD: 3/10; OS: 2/10 | 4 | 1 |
| 8 | Male | 75 | Married | Elementary | Self-employment | OD: 1m CF; OS: LP | 24 | 11 |
| 9 | Male | 59 | Married | Elementary | Self-employment | OD: 3/10; OS: 4/10 | 1 | 0.5 |
| 10 | Male | 55 | Married | Middle school | Self-employment | OD: 2/10; OS: 4/10 | 2 | 0.5 |
| 11 | Female | 75 | Married | Elementary | Housewife | OD: 1m CF; OS: LP | 30 | 13 |
| 12 | Female | 40 | Married | Bachelor | Nurse | - | - | - |
| 13 | Female | 36 | Married | Master of science | Nurse | - | - | - |
Demographic Characteristics of Participants
4.1. Main Category - Improving Access to Comprehensive Care
Data analysis led to the main category of "improving access to comprehensive care," four categories, and 14 sub-categories (Table 2).
| Main Category | Categories | Sub-categories |
|---|---|---|
| Improving access to comprehensive care | Receiving preventive care | Screening |
| Disease control | ||
| Support | ||
| Consulting | ||
| Access to home care | Improving self-care | |
| Continuity of care | ||
| Reduction of dependence | ||
| Safety promotion | Lifestyle modification | |
| Optimizing the treatment plan | ||
| Management of health threats | ||
| Increasing health literacy | Need-based education | |
| Access to information | ||
| Understanding and correct application of education | ||
| The ability to decision making |
Main Category, Categories, and Sub-categories Extracted from the Experiences of Participants
4.2. Receiving Preventive Care
One of the consequences of meeting health expectations stated by participants was receiving preventive care. The participants suggested health centers conduct counseling and screening programs and pay attention to patients' expectations in this field. One of the participants said, "I wish health centers would have given me the necessary consultations on diabetes prevention before" (P5). The patient's nurse said, "First-level care is very important in the community, and the health system should pay special attention to this and reduce the workload and costs in the system by promoting the health of the community and preventing diseases" (P13).
The participants also stated that another consequence of meeting expectations is receiving care for disease control and preventing diabetes complications, especially vision disorders. In fact, paying attention to the expectations and needs of patients leads to improving health, supporting the patient, and providing nursing care to control disease and prevent complications. According to them, the health system should take measures to control diabetes and prevent complications, and they emphasize the important role of nurses in this field. The following quotations reveal some of the concerns of patients:
"I expect to have access to my doctor and nurse if needed and to be at my bedside on time" (P8). The patient's companion said, "I wish the Ministry of Health would consider a place for diabetic patients and that diabetic patients would go there to control their disease and not suffer from complications like this. It is so bad that we seek treatment after complications occur" (P2).
4.3. Access to Home Care
Access to home care was another participant's expectation. Since patients with diabetes suffer from many problems, including vision disorders, they may have problems taking care of themselves at home. They have to run errands, prepare their diabetes medication, inject their insulin, monitor and record their blood sugar, and take care of themselves; however, they cannot take care of themselves, and as a result, the treatment process is disturbed. The participants emphasized the role of nurses in improving patients' self-care activities and reducing their dependence on the health system. They also pointed out the importance of follow-up of patients and continuity of care at home by nurses and expressed it as a factor in improving health. According to them, by examining the expectations and needs of the patients, these cases can be determined, and the necessary measures can be taken. The following quotations reveal this:
"Many times I could not inject my insulin, and there was no one to help me. I'm afraid that my condition will get worse and I won't be able to take care of myself anymore" (P1). The patient's companion said, "My mother is alone at home and needs care and support. My mother cannot control her blood sugar. If she could control her blood sugar well, she would not be in this condition now" (P2) and said: "Health staff should not leave the patient after discharge from the hospital and it is better to follow them in different areas including educating, problem-solving and answering their questions" (P2).
4.4. Safety Promotion
Safety promotion includes lifestyle modification, treatment plan optimization, and health threat management. Patients with DRVI should be able to change their lifestyle and take steps to improve their treatment plan, including proper nutrition, exercise, and maintaining blood sugar within the normal range. They should also be able to identify and manage health threats, including possible leg ulcers, vision disorders, and blood sugar fluctuations. The participants of the present study also pointed to the achievement of these goals and called the role of nurses important in achieving these goals. The following quotations reveal this:
"If I know how to manage diabetes and its complications, I can take better care of myself" (P8). "I know that exercise is useful for me, but I don't know how to exercise, and I don't have a place to exercise" (P3). "I wish I knew in advance how to prevent the progression of my blindness. My nurse could have helped me more in this matter" (P5). Another participant said, "I don't know what I should have done so that I wouldn't have diabetes, and I don't know what I should do now so that my condition doesn't get worse" (P11).
4.5. Increasing Health Literacy
Increasing health literacy refers to need-based education, access to information, understanding and correct application of educational items, and the patient's decision-making ability. Patients with DRVI, like all patients with chronic diseases, need education and access to information to make good decisions about the problems caused by the disease and prevent the disease's progress. Of course, increasing health literacy in these patients is more important than in other chronic diseases due to the involvement of multiple physical and mental systems.
Since increasing health literacy is important for all chronic diseases, especially diabetes, this was also noted by the participants in our study. The participants asked the nurses to examine the patients' needs and provide the necessary training according to the cultural and social context and literacy level. One of the participants said, "I want nurses to provide me with proper training by examining my training needs" (P4). Another participant emphasized the nurses' attention to the patient's literacy level during training and said, "When teaching, nurses should pay attention to the literacy level of each patient and provide education based on their literacy level and individual understanding. During my training, my nurse used medical terms that I did not understand" (P7). Another participant said, "If I get enough training and if I get more information about diabetes and my eye problems, I can control my disease better" (P5).
5. Discussion
The high burden of diabetes (approximately 90% of the estimated 537 million) and the presence of multiple diseases for most diabetic patients are recognized globally (30). The results of this study showed that including patients' perspectives can be effective in improving the care process. Patients can better help us in the field of care and services due to their knowledge of the disease and the problems caused by it. By considering the perspective of patients with DRVI, we can provide comprehensive and patient-centered care as one of their basic rights and improve their health outcomes (30). An innovative approach to health care, patient-centered care strengthens the independence and empowerment of patients and their families while respecting their values and beliefs (31).
Patients with DRVI need comprehensive care based on individual needs due to numerous physical and mental problems (30, 32, 33). In this study, "improving access to comprehensive care" was extracted as the main consequence of meeting health expectations in visually impaired patients caused by diabetes. In this main category, the categories of "receiving preventive care," "access to home care," "safety promotion," and "increasing health literacy" were included.
Receiving preventive care was one of the sub-categories of the main category, "improving access to comprehensive care," in patients with DRVI. Prevention of diseases, especially diabetes, is emphasized in all literature. Seidu et al. emphasized the importance of diabetes prevention (30). The participants in our study also emphasized this issue and called for prevention before the disease occurred.
Controlling diabetes is very effective in preventing complications of the disease. In the present study, the participants requested the control of diabetes, prevent complications, and achievement of comprehensive and patient-centered care. Authors have also mentioned this important issue in their studies and considered disease control as a factor for maintaining patients' health (30, 32, 34). Escudero-Carretero et al. stated in their study that the treatment of patients with diabetes should be monitored daily (34). In the study conducted by Halperin et al., patients requested an informed, caring, accessible and well-communicated team that can control diabetes (effectively, patient-centered and timely) and prevent diabetes complications (35).
Access to home care was another sub-category that emerged from patients' experience with DRVI in the present study. Home care and continuity of care are important for patients with chronic diseases. Home health care includes 24-hour access to various health and social services at home. These cares are provided when the patient needs health care after being discharged from the hospital or prefers to be cared for at home (36). Unfortunately, in the health system of Iran, hospital-based services are preferable to community-based services, which have no position in Iran's health system. While with the change in demographic characteristics, authorities in the world have been forced to use community-based care, and most European countries have prioritized home care in their healthcare system. In Iran, too, due to the high statistics of chronic diseases, the health care system needs fundamental reforms (37). In this regard, Naithani et al. emphasized the continuity of care for patients with diabetes from health centers to home (38). In the study of Jacklin et al., participants felt satisfied with health professionals' communication and their follow-up in care (39). The importance of this issue is so much that the patients in our study mentioned it and pointed out their inability to take care of themselves. Therefore, to provide comprehensive care to patients with low vision due to diabetes, the healthcare team should consider their follow-up and continuity of care at home.
Self-care and reducing dependence on the healthcare team and the family are very important for chronic patients, especially with diabetes. The American Diabetes Association has emphasized promoting self-care and self-management of patients in order to prevent the complications of diabetes (32). In various studies, self-care promotion has been mentioned as the expectations and consequences of meeting the needs of patients with diabetes (34, 40-42). In the present study, the participants also pointed out the importance of self-care and its promotion and emphasized the role of nurses in this issue.
Safety promotion, which refers to modifying lifestyles, optimizing treatment plans, and managing health threats, was one of the extracted categories in this study. Lifestyle management is a fundamental aspect of diabetes care and includes diabetes self-management, nutritional therapy, physical activity, smoking cessation, and psychosocial care (43). In the study by Halperin et al., the participants stated that the most important consequence of meeting their expectations was improving safety. In addition to the expectation of avoiding diabetes complications, the safety concern that patients in this study most emphasized included avoiding hypoglycemia and side effects of the drugs (35). Grund and Stomberg’s study results show that the patient strives towards competence and self-confidence to balance lifestyle and blood sugar normalization (44). From the results of various studies and the present study, it can be emphasized that the most important concern of patients with DRVI is in the field of safety. If the health system pays attention to these expectations, the patients will feel satisfied and access comprehensive care.
Another consequence of meeting expectations in patients with DRVI in the present study was increased health literacy. Continuous education and self-management support for diabetic patients is crucial to preventing early and long-term complications (32). One study result has shown that patients are deprived of adequate and appropriate education in diabetes control and blood sugar control (33). Patients with DRVI should be able to use the information obtained during their health care and make decisions related to their health using the available information. In the present study, patients pointed out the lack of sufficient education in the field of diabetes to prevent complications, and they considered the role of nurses important in providing education to patients. In various studies, researchers have emphasized the importance of patients' education about diabetes (32-34, 36, 41). Yao et al. mentioned increasing awareness in the field of diabetes, prevention of its complications, and self-management education (42). In most studies, only the education of diabetic patients is emphasized, and the ability of patients to use information and decision-making in the field of health care is not mentioned; while in the present study, in addition to training and receiving information, the participants emphasized the necessity of their ability to use the information obtained in the field of health.
As can be concluded from the results of various studies, examining and meeting the expectations of patients with diabetes- related visual impairment will have positive results for patients and the health care system. However, more studies are needed in this field, especially in this country.
One of the limitations of this study was that it was conducted in the specific cultural and social context of Iran, so further interpretation of the study results must be made with caution.
5.1. Conclusions
Overall, the results of this study showed that receiving comprehensive care based on individual needs and patient-centered care is the most important consequence of paying attention to the expectations of patients with low vision due to diabetes. This means that if the health care team, especially nurses, examines the needs and expectations of these patients and takes action to solve them, they will help to provide quality care based on the individual needs of the patient. Therefore, it is better to examine the needs and expectations of these patients early and include them in the list of nursing interventions. Obviously, increasing these patients' satisfaction and improving their level of health will increase the credibility of the healthcare centers. Also, the results of this study showed a big gap between the needs and expectations of patients from the health system and the services provided. Therefore, the attention of health policymakers and nursing managers is emphasized on this issue. Also, the importance of paying attention to patients' expectations to improve the overall health of society and the satisfaction of patients should be included in the educational content of students.
