






1. Background
As a common worldwide phenomenon, it’s necessary to consider substance abuse as one of the most prominent social problems that simply expose the foundation of the personal, family, and social life of the individual and society to disintegration (1). Unfortunately, the number of people with an addiction suffering from negative outcomes of addiction (including the physical, psychological, economic, and social consequences) is increasing (2). Collegegoers, like other classes of society, are prone to substance abuse (3). The academic period of life is associated with educational pressures, a sense of separation from family and loneliness, limited parental supervision, entering a large and stressful community, and the fear of experiencing new and unknown conditions, and the university provides a new social environment where alcohol and drugs are commonly abused for recreational purposes (4, 5). Amid this, the students of medical universities are at greater risk for substance abuse due to their greater familiarity with and access to drugs (6). Substance abuse among young students is an extremely sensitive issue since they are the main core of human resources in any country and play a remarkable role in the development and elevation of that country. On the other hand, substance abuse by the youth imposes huge costs on society. It accompanies social, psychological, health, and economic burdens on society (7).
Today, efforts keep going to find the underlying causes of substance abuse. In this regard, the role of cognitive and psychological factors in this phenomenon has been critical. Many researchers concentrated on studying the attitude and role of dysfunctional beliefs in substance abuse. These studies have emphasized the role of positive and negative attitudes. People's attitudes, personality traits, and demographic factors are distinctive in correcting and reinforcing negative attitudes toward substance abuse (8, 9). Today, the role of misconceptions is stressed in various aspects of life, particularly education (10-12). Misconceptions are the basis of insufficient and false knowledge and can be the source of behavior. In this respect, the role of common misconceptions is important, especially in substance abuse. The existence of misconceptions about substance abuse is prevalent, and therefore, identifying the common types of such misconceptions can pave the ground for changing substance abuse behavior because the presence of such misconceptions can lead to substance abuse among people, in particular students (13, 14).
Accurate understanding serves as a foundation for inclusive learning of new information and provides a framework for the development of higher-level conceptual knowledge. The importance of misconceptions in science education has been stressed in the past three decades (15). Misconceptions are immature understandings in conflict with the currently accepted concepts and empirical findings. They are often strongly held and are thus resistant to correction (16). Misconceptions may act as a trigger for substance abuse behaviors. In education, being aware of misconceptions is one of the most important skills in student education (15). In addition, some measures can be taken to correct them merely by identifying their natures (17). Pursuant to prior studies, misconceptions exert a huge impact on students' educational performance; however, no study has empirically examined the common types of misconceptions about substance abuse among students (16).
Many studies acknowledged the high prevalence of substance abuse in Iran and the world (18-20). The results of one study conducted in Iran implied that abusing various substances among Tehran-based students is more than 10%, with the highest frequency of abuse in the boys of the technical and engineering department at 30%. Moreover, 73% percent of abusers were non-native, and 45% of them lived in dormitories (19). A Canadian study similarly indicated that a large number of young Canadians abuse alcohol, tobacco, marijuana, and illegal substances (21). Abusing psychoactive and laboratory substances such as crystal among the student population leads to deleterious socioeconomic and psychophysiological consequences, including lack of academic motivation, academic failure, dangerous driving, crime and theft, poverty and loneliness, suicide, aggressive behaviors, a sense of identity loss, high-risk sexual behaviors, mood disorders, and depression, sleep and appetite disorders, and wasting macro material capital and the human resources (2, 22).
However, no standard tool has been found via searching the available databases in order to investigate the common types of misconceptions about substance abuse among the students. Considering this, it is necessary to identify the types of such misconceptions so as to build the appropriate interventions for changing them.
2. Objectives
The current study was designed and carried out to design and psychometrically examine an inventory of the common types of misconceptions among students about substance abuse.
3. Methods
3.1. Type of Study
This methodological study is part of a master’s thesis conducted from May to November 2019. The current research was carried out in two phases (an inductive phase followed by a deductive phase) with the objective of designing and psychometrically evaluating students’ common types of misconceptions regarding substance abuse pursuant to the method of Waltz and Basel (2010). In the first phase, a conventional content analysis was performed, and the items were generated. Using the exploratory factor analysis (EFA) and confirmatory factor analysis (CFA), the construct validity was examined in the second phase.
3.2. First Phase
3.2.1. Item Generation
In the first phase, the participants' common types of misconceptions regarding substance abuse were extracted based on conventional content analysis. The participants were selected using purposive sampling among the medical substance-abusing students who were referred to the university counseling center. The inclusion criteria were as follows: Willingness to cooperate in the study, the ability to understand and speak Persian, and the physical ability to participate in the study. The interviews with the selected participants were conducted by two researchers. Maximum variation in terms of education and age was done in selecting the samples. The common types of misconceptions in terms of substance abuse were explored by semi-structured interviews. The semi-structured interviews were conducted by posing the following questions:
- What do you think about substance abuse?
- In spite of this fact being proved that addiction is an unpleasant behavior and an action that results in negative consequences, what made you resort to substance abuse?
For more probing, some other questions, such as “what do you mean?" or "how did you feel about that issue?" were also posed.
Each interview lasted 20 - 30 minutes. All interviews were held by the same interviewer in Persian language. Then, the recorded interviews were transcribed verbatim and read several times. Based on the Graneheim and Lundman method, data analysis was performed by conventional content analysis. The meaning units were selected according to the study goal, and then the initial codes were extracted. The codes were classified based on their similarities as subcategories and similar subcategories were allocated to a single category (23).
3.2.2. Trustworthiness of Data
For confirming the trustworthiness of data in the qualitative phase, Lincoln and Guba’s evaluation criteria (i.e., credibility, confirmability, dependability, and transferability) were employed (24).
The continuous involvement of researchers in data collection facilitated the acquisition of credibility. For confirmability, the researchers reserved all the documents of the study, and detailed reports were provided. Moreover, the research team repeatedly read the entire transcriptions, the initial codes, and the categories. The findings also were checked by the participants. Depending of the data, the codes were reviewed through a member check and then by an external checker. To ensure data transferability as much as possible, the participants were selected from diverse backgrounds, and a thorough description of the study method was presented (24).
3.3. Second Phase
To create a set of preliminary items, the deductive method used in this phase provided sufficient information. This deductive method provided an understanding of the concept under study, and the literature review delivered a theoretical definition of the construct under study. Additionally, for designing the questionnaire, it is recommended to review the relevant literature, related theories, and their methods regarding the studied phenomenon (25).
In the first phase, the related literature in Iran and other countries was reviewed. The present study keywords were ‘attitude’, ‘misconception’, ‘myth’, ‘substance abuse’, ‘medical Students’, and ‘student’, which were searched in the databases, including PubMed, Scopus Irandoc, Magiran, SID, and Google Scholar, with no publication time limit.
3.4. Third Phase
3.4.1. Item Reduction
In this step, after the integration of the qualitative and literature reviews, the pool of items was provided. Based on the results of the first stage, among the 250 initial codes, the 6 categories from the misconceptions were: (1) misconceptions based on the therapeutic role of substances; (2) misconceptions based on the positive and pleasant effects of substances; (3) misconceptions based on the situations of use; (4) misconceptions based on the difficulty quitting drug addiction; (5) misconceptions based on the moral and social dimension of substance abuse; and (6) misconceptions that block the therapeutic action.
The initial 71-item questionnaire was revised in several meetings in terms of writing, clarity, relevancy, and specificity for each component. Some misconceptions about substance abuse extracted from the interviews and literature review are presented in Table 1, and an example of the items formation process is given in Table 2.
| Some Misconceptions Extracted from the Interviews | Some Common Misconceptions About Addiction Extracted from the Literature Review |
|---|---|
| If quality substances are used, they are not addictive. | I can quit my addiction whenever I desire. |
| Consuming substances like cannabis causes addiction. | Prescription drugs (substances) are not addictive like street drugs because of being prescribed by a doctor. |
| If a substance is used in small amounts, it is not addictive. | Addiction is just about drugs and alcohol. |
| Substances like opium can have medicinal effects. | If someone has a stable job and family life, they can’t be suffering from addiction. |
Some Misconceptions Extracted from the Interviews and the Literature Review
| Item | Category | Code | Items Codified Based on Participants' Interviews |
|---|---|---|---|
| Substance abuse is suitable for the treatment of some diseases. | The medicinal effect of substances | The medicinal effect of substances | Some expert doctors also use substances like opium. If the substance is bad, it is not used for some diseases. Taking drugs for some diseases has a medicinal effect. |
| In happy times, substance is a good thing; if substances are pure and of good quality, they are not addictive and have no side effects. | No addiction with a small amount of drug consumption | Abusing substance with good quality; consumption of substance in a small amount; refreshing by substance abuse | If something has quality, it is good to consume. The same is true for substances; when they are of high quality, you will not become addicted. Consuming substances in a small amount at a party or in the company of friends does not lead to addiction, and the person gets refreshed. |
An Example Representing the Process of Item Formation
The second stage involved quantitatively evaluating the instrument, which included assessing face validity (both qualitatively and quantitatively) and content validity (both qualitatively and quantitatively, as calculated by content validity index (CVI) and content validity ratio (CVR)). The construct validity was examined by EFA and CFA with two 375 samples for each of them and reliability.
3.5. Face Validity
In the study, the qualitative and quantitative face validity was assessed. Face validity deals with whether a measure appears relevant and appropriate for what it is ostensibly assessing (26). To assess the face validity qualitatively, 10 medical sciences students were asked to rate the level of difficulty, the degree of appropriateness, and ambiguity of the scale items. Item Impact Score was calculated to determine quantitative face validity for all items. Thus, the same participants rated the importance of each item using a 5-point Likert scale (absolutely important-absolutely unimportant).
Item impact score was calculated by the formula below:
Item impact score = Frequency (%) × Importance
Content validity assesses the relevance of the content and the purpose of an instrument. In the study, the qualitative and quantitative content validity were assessed. The qualitative content validity was evaluated by 10 experts in psychiatry, psychology, and psychiatric nursing. The items were evaluated in terms of grammar, the right words, representations, clarity, and being properly placed. Content validity ratio and CVI were measured to assess the quantitative content validity:
To calculate the CVR (content validity ratio), the Lawshe table (1975) was applied (27). To determine the content validity ratio, ten experts in psychiatry, psychology, and psychiatric nursing evaluated a 71-item questionnaire in terms of necessity and on a three-point Likert scale.
The content validity ratio formula is:
Subsequently, 45 items with scores of 0.62 and higher were accepted as the items with a suitable content validity ratio according to the Lawshe table.
Content validity index: The content validity index of the instrument was measured in terms of three criteria, i.e., simplicity, relevance, and clarity, according to the Waltz and Bausell’s method (28) and in a four-point Likert scale by 10 experts (those who assessed the instrument's CVR). In this study, a CVI score higher than 0.78 was considered appropriate, and the items with a lower score were excluded (29).
In the end, according to the Lawshe table, 30 items scored 0.62 and higher, the content validity index higher than 0.79, and the acceptable impact factor of the item was employed as the suitable items for conducting the next stages of psychometric evaluation.
3.6. Construct Validity
First, the EFA was also used to measure the construct validity.
At this stage, the samples were selected conveniently. In this study, the number of samples was 10 participants per item of the instrument (30), and at least 300 main participants were selected randomly for both psychometric evaluation stages. In order to analyze the data, the data set (n = 750) was randomly divided into two datasets. The first data set (n = 375) was applied for exploratory factor analysis using SPSS-27, and the second data set (n = 375) for confirmatory factor analysis by AMOS-27.
In order to analyze the data, the data set (n = 750) was randomly divided into two datasets. The first data set (n = 375) was applied for EFA using SPSS-27, and the second data set (n = 375) for confirmatory factor analysis by AMOS-27. To outline the questionnaire’s structure, the maximum likelihood (ML) estimation method and Promax Rotation and Kaiser-Meyer-Olkin (KMO) > 0.8 were employed by exploratory factor analysis. Bartlett's Test of Sphericity was significant (P < 0.05) and showed relevance and appropriateness of the data. The factorial structure of the misconceptions inventory on substance abuse was followed with the eigenvalues > 1, commonalities > 0.2, and scree plots. In the extracted factors, the factor loading for each item was more than 0.3.
Confirmatory Factor Analysis: In the next stage, to validate the factorial structure extracted from EFA, the maximum likelihood of CFA was conducted. In this stage, fit indices of modified model confirmatory factor analysis of the common types of misconceptions among the students were assessed (Table 3). This study also assessed the internal consistency (Cronbach’s alpha). The acceptable Cronbach’s alpha should be greater than 0.7.
| CFA Index | Modified Model |
|---|---|
| (χ2) | 283.404 |
| χ2/df | 2.959 |
| GFI | 0.912 |
| NFI | 0.927 |
| IFI | 0.909 |
| TLI | 0.934 |
| RMSEA (90% C.I.) | 0.047 (0.045, 0.071) |
Fit Indices of Modified Model Confirmatory Factor Analysis of the Common Types of Misconceptions Among the Students
In this study, the normality of the data was evaluated in univariate and multivariate forms. The outliers, skewness, and kurtosis were assessed for univariate distributions. In addition, Mardia’s coefficient > 8 indicated a departure from multivariate normality. Furthermore, using the Mahalanobis distance (P < 0.001), the outliers of the multivariate were detected.
3.7. Reliability
The internal consistency and stability were used to check reliability (31). Cronbach's alpha was calculated to measure the homogeneity or internal agreement. The acceptable Cronbach’s alpha should be 0.7 or more. Test-retest reliability was also used to analyze stability. In this research, the instrument was repeated at two different times (within a two-week interval) in the same samples. Then, the intra-class correlation coefficient (ICC) analysis was performed regarding the scores of the two tests. Intra-class correlation coefficient = 0.8 - 0.9, which indicates decent reliability, was taken into account (32).
3.8. Scale Scoring
The most common response format used in the design of attitudinal or behavioral instruments is the Likert scale. The Likert scale is simple to construct and presumably suitable to produce a reliable scale. Besides, it is easy to read and complete (33). For this instrument, the Likert scale was used and rated on a 5-point Likert scale (strongly disagree- strongly agree). The scores achieved on the scale ranged from 16 to 80.
3.9. Data Analysis
In the second phase for EFA and CFA, other analyses, namely SPSS-27 and AMOS-27, were used, respectively. The Mardia’s coefficient > 8 was assessed for multivariate normality of data.
3.10. Ethical Considerations
The present study with the ethics code IR.MAZUMS.REC.1399.421 was approved by the Research Department of Mazandaran University of Medical Sciences (MAZSUMS). The participants signed a written informed consent form. The right to anonymity and confidentiality of information and the right to decide to leave the research at any time of the study were also respected.
4. Results
In the current study, 750 Iranian students (MAZSUMS) participated, where the mean (SD) age of the participants was 22.59 ± 5.28 y., and 54.6% (n = 423) of them were women. They studied medicine (n = 292, 38.9%), pharmacy (n = 55, 7.2%), nursing and midwifery (n = 137, 18.2%), allied medical sciences and advanced technologies in medicine (n = 173, 23%), health (n = 47, 6.26%) and dentistry (n = 46, 6.13%) colleges.
The results of exploratory factor analysis on the misconceptions inventory on substance abuse are shown in Table 4. In the study, the factor analysis was performed according to KMO = 0.881, and a significant Bartlett's Test of Sphericity (P < 0.001, 4024.244, df = 120) indicated the relevance and appropriateness of the data. Three factors, including 16 items and 40.86% of the total variance, were extracted. Satisfactory internal consistency and construct reliability were demonstrated by Cronbach’s alpha coefficients greater than 0.7 for all factors.
| Factor | Items | Factor Loading | h2 | λ | Variance (%) | Internal Consistency | |
|---|---|---|---|---|---|---|---|
| Factor 1: Borderline misconceptions | q22 | Opium, cannabis, and plant-based substances are not harmless because they have plant origins. | 0.888 | 0.689 | 2.845 | 17.78 | α = 0.804 |
| q28 | Consumption of small amounts of substances is not addictive. | 0.887 | 0.730 | ||||
| q29 | If the substances are pure and of good quality, they are not addictive and have no side effects. | 0.830 | 0.695 | ||||
| q8 | Taking some substances, such as cannabis and flowers, does not cause addiction. | 0.676 | 0.538 | ||||
| q4 | Only substances such as heroin, morphine, and amphetamines cause addiction. | 0.352 | 0.218 | ||||
| Factor 2: Positive effects based misconceptions | q25 | Substance abuse leads to creativity. | 0.668 | 0.352 | 2.352 | 14.7 | α = 0.746 |
| q16 | Substance use is suitable for the treatment of some diseases. | 0.636 | 0.343 | ||||
| q20 | Substance abuse increases sexual potency. | 0.558 | 0.285 | ||||
| q23 | Medications prescribed by a doctor do not cause addiction. | 0.490 | 0.398 | ||||
| q17 | Substance abuse has healthy effects. | 0.451 | 0.236 | ||||
| q18 | Substance is cure | 0.439 | 0.352 | ||||
| q11 | Taking Substances during times of sickness is not harmful. | 0.408 | 0.213 | ||||
| q7 | Only some people are at addiction risk. | 0.388 | 0.352 | ||||
| Factor 3: Situational based misconceptions | q2 | Sometimes, in the company of friends, substance can be used. | 0.741 | 0.508 | 1.341 | 8.38 | α = 0.701 |
| q5 | In happy times, substance is a good thing. | 0.701 | 0.515 | ||||
| q13 | We do not get addicted when taking them recreationally. | 0.549 | 0.464 | ||||
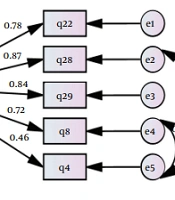
In the next stage, to validate the factorial structure resulting from EFA, maximum likelihood CFA (n = 375) was performed. As demonstrated In Figure 1, three pairs of measurement errors were acceptable to freely co-vary (e2 to e5, e4 to e5, e6 to e9, e7 to e8, and e7 to e9) to improve the model.
 for substance abuse misconceptions among the students")
The conformity factor analysis (measurement model) for substance abuse misconceptions among the students
The factor loadings ranged from 0.44 to 0.87 for all items and were considered significant. These parameters are presented in Table 3.
5. Discussion
The current study was conducted to design and psychometrically evaluate the students’ common types of misconceptions about substance abuse inventory. The results indicate that the three-factor inventory designed to assess common substance abuse misconceptions has acceptable validity and reliability. The instrument was designed using both inductive (qualitative) and deductive (literature review) methods and consisted of 16 items. It is important to note the instruments with fewer items are less likely to cause respondent fatigue. In the current study, the first domain consisted of five items, the second domain consisted of eight items, and the third domain consisted of three items. The use of both qualitative and quantitative methods is important to ensure the validity and reliability of the instrument. For face and content validity, both methods were used. To assess content validity qualitatively, the experts were asked to review the scale, and then the suggested corrections were made. Factorial analyses were done to determine the domains of the instrument and confirm the validity of the construct.
In designing an instrument, it is important to consider its psychometric characteristics, which are validity and reliability. To ensure the validity and reliability of an instrument, both qualitative and quantitative methods should be considered (34).
In this study, these two psychometric characteristics were studied. In the first, the experts were required to review the inventory to determine content validity qualitatively. It is important to note that quantitative methods should not replace qualitative methods for investigating content and face validity. Both methods should be used together to ensure the validity of the study (35). The use of both quantitative and qualitative methods can help to ensure the rigor and robustness of the research process and results. It is also important to consider the epistemological and philosophical paradigms of the research when evaluating the quality of the study (36). This study conducted both exploratory and confirmatory factor analyses. Prior to EFA, results of the two tests, the KMO = 0.88 and Bartlett's Test of Sphericity (P < 0.001), revealed that factorial analysis can be used to identify the structure of the model. The CFA was conducted with a sample size of 375 to validate the factorial structure obtained from the EFA. The results of the CFA were evaluated using several fit indices. The chi-square (χ2)/degree of freedom (df) ratio was less than 4, which shows that the model had good fitness. The RMSEA value of 0.047 was considered good, as it was less than 0.05 (25). In addition, the values of indices of fitness of the modified model were all greater than 0.9, confirming the model’s fitness. It’s worth stating that the significance of the chi-square test should be interpreted with caution, especially in small to medium sample sizes (37). This study showed acceptable Cronbach’s alpha coefficients for all factors (α ≥ 0.7) (38).
Theoretically, these misconceptions can serve as a reinforcing factor for substance abuse, and due to these misconceptions, the stigma of substance abuse disappears, and they can promote substance abuse. Also, a study done by Yigitoglu and Keskin concluded that substance abusers have dysfunctional beliefs and exhibit emotion-focused coping attitudes. They theoretically reasoned those dysfunctional beliefs could generate maladaptive coping attitudes, and they may result from substance abuse behavior (39).
One of the three main types of misconceptions is borderline misconceptions. The items related to this type encompass cases such as plant versus chemical origin, consumption of small versus large amounts, purity or impurity, cannabis, and some flowers and non-cannabis being conceived as the border of healthy or unhealthy substances. A study also revealed that substance abusers perceived both the positive and negative effects of substance abuse. This study reported two positive effects: The self-regulation effect on physical and behavioral health and also on feelings-thoughts-reasoning and the rewarding effect. Additionally, its negative effects were perceived as the negative consequences of substance abuse on health (40).
Another type of misconception is about the perceived positive effects of substances. Theoretically, this type confirms the misconceptions emphasizing the existence of substance-induced positive effects. On the other hand, a study also verified that the perceived negative effects of drugs among young people and teenagers can be one of the factors preventing them from substance abuse (41). A qualitative study about the positive and negative aspects of substance abuse and treatment goals among the patients suffering from substance abuse disorder (SUD) with and without attention deficit hyperactivity disorder (ADHD) showed that the perceived positive aspects of SU among the SUD+ADHD patients were less frequent (36). These misconceptions are prevalent among substance abusers, which can be induced by possible factors including lack of interest in learning about drugs, low self-esteem, feeling no demand for information, denying the risks associated with substance abuse, and not being familiar with the sources of gaining information about substances (42).
The third type of misconception emerging in this research is “situational misconceptions”, which refers to social situations in which substance abuse does not cause problems. Some studies have emphasized the role of social context in substance abuse behavior (43, 44). Dysfunctional beliefs not only promote substance abuse but also involve individuals in high-risk situations and substance abuse relapses (45). Therefore, situational misconceptions revealed the role of social context that could be important in the tendency to substances. Besides, the inconsistencies in the findings related to the relationship between substance abuse and personal factors highlight the role of contextual factors, such as the sociocultural factors associated with substance abuse (44). In addition, a study suggested that the social contexts of substance abuse vary according to the type of substance, and the most common situations to use alcohol, marijuana, and multiple drugs were parties. At the same time, nonmedical abuse of prescription stimulants, sedatives, and opioids was most likely to occur at home. Most incidences of substance abuse occur in the presence of other people, except for the nonmedical abuse of prescription stimulants, which are used alone (46). In the results of our study, "situational misconceptions" may trigger substance abuse behavior. In another study in Iran, Rahmati and Pourehsan designed an instrument to measure the attitude toward drugs among the students of Shahid Bahonar University in Kerman. Their instrument included three cognitive, emotional, and behavioral factors (47).
The current study revealed three types of misconceptions encompassing borderline misconceptions, positive effects-based misconceptions, and situational misconceptions. In a study with the objective of determining the knowledge, attitude, and performance of substance abuse among teenagers and young people in schools and universities, the results indicated that defective knowledge, a tendency to a risk-taking attitude, and various ways of substance abuse pave the ground for the tendency to substance abuse among the mentioned groups (48). Theoretically, defective knowledge of substance abuse can be the foundation of such misconceptions.
However, this research was conducted on medical students with a larger sample size and via a factor analysis method with more acceptable reliability and validity and with fewer items, which makes it easier to use for large-scale national research.
5.1. Limitations and Strengths
Among the limitations of the present study, we can point out the validation stages of this study, which was conducted merely on medical students, which limits its generalizability to the entire society, including adolescents and adults. Therefore, it is imperative to focus on investigating the common types of misconceptions in terms of group diversity and age in future studies. This study was conducted in Mazandaran province (located in the central-northern part of Iran), and it is recommended to be replicated in other cultural contexts in Iran.
5.2. Conclusions
Pursuant to the current study-derived results, the final model included three main factors, namely, borderline misconceptions, positive effects-based misconceptions, and situational misconceptions, which matched well with the data after checking the correction indicators. Moreover, the common types of substance abuse misconceptions scale showed the required necessary validity and reliability to investigate and evaluate the common types of misconceptions among the students. On the other hand, this inventory is congruent with Iranian students' culture, and it is lucid for responding. Moreover, in order to promote students’ health, effective health preventive strategies, including drug preventive programs, should be implemented. The psychometric tool applied in this study can lead to the implementation of more effective and evidence-based programs to prevent substance abuse among students.
