



1. Background
In recent years, fertility rates have significantly declined, while life expectancy has risen, particularly in developing countries. The long-term effects of population aging include slower economic growth, a reduced labor force, and higher elderly care costs (1-4). In response, the Iranian government has implemented fertility protection policies, offering economic and social incentives and limiting access to contraceptives (5, 6). However, these policies have faced resistance from many couples (7).
Health education has gained considerable attention for its positive impact on various health outcomes (8). In Iran, the popularity of distance education, especially through virtual platforms and mobile phones, surged during the COVID-19 pandemic (9, 10). Research has demonstrated the effectiveness of virtual education in promoting health-related behaviors (6, 11). For example, Daniluk and Koert found that virtual educational programs improved fertility awareness and influenced perceptions regarding the optimal timing for childbirth (6). Other studies have shown that virtual education enhances fertility knowledge, attitudes, and counseling skills among healthcare professionals (11).
Mobile phone technology has also transformed the education and healthcare sectors by introducing new educational methods that differ from traditional approaches (12). Studies have shown that mobile-based education improves self-care behaviors in patients with type 2 diabetes (13), promotes mother and child health (14), and raises awareness about glaucoma (15). Mobile technology allows education to be accessible at home, at work, and even while traveling. Despite its effectiveness, the results of using this method for certain health concepts remain ambiguous (16).
However, there is a notable gap in empirical research specifically examining the impact of Internet-based education on fertility knowledge and its influence on childbearing decisions. While general health behaviors have been studied extensively, the direct relationship between virtual education and attitudes toward childbearing remains underexplored.
Attitudes play a critical role in shaping intentions and behaviors, particularly in the context of childbearing, making the selection of appropriate educational methods essential. Research indicates that education significantly affects attitudes towards childbearing (17, 18). Nevertheless, there is still a lack of understanding regarding which educational methods are most effective in influencing these attitudes. This study seeks to address these gaps by comparing the effectiveness of telephone-based and virtual education in shaping women's attitudes toward childbearing.
2. Objectives
By analyzing these two distinct educational mediums, this research aims to provide valuable insights into the potential impact of different training approaches on key health-related perspectives, thereby informing future educational strategies and policy decisions.
3. Methods
This interventional study, conducted from May 2021 to September 2021, targeted three groups of married women in Babol city, Mazandaran. Babol, a major city in northern Iran with over 250,000 residents, is well-equipped with comprehensive healthcare centers. The inclusion criteria required participants to be 18 - 35 years old, nulliparous, literate, in possession of a smartphone, not using drugs or alcohol, and free of mental disorders or conditions affecting pregnancy. Participants were allowed to withdraw from the study if they chose not to continue or if they decided to engage in parenting classes.
3.1. Sample Size and Sampling Method
The sample size was determined considering a 95% confidence level, 80% test power, a first-type error of 5%, an approximate standard deviation of 22.5, and an effect size of 0.58, as derived from previous studies (19). The sample size was calculated to be 145, and assuming a 20% dropout rate, 174 women (58 in each group) were included. This resulted in a calculated sample size of 46 individuals per group, with 58 participants allocated to each group to account for possible dropouts.
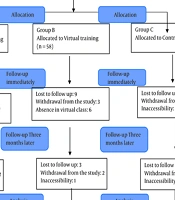
A multi-stage cluster method was used for sampling. First, the number of comprehensive urban health centers in the four geographic regions of North, South, East, and West of Babol city was determined by an expert from the health extension unit of Babol University of Medical Sciences, according to the city map. Comprehensive health centers with larger populations were selected from each region. The number of households within these centers was divided by the total number of households in Babol, and the result was multiplied by the required sample size. This process, employing probabilities proportional to size, yielded the necessary number of samples for each urban base. To randomly allocate the samples, a six-block method was used. A sequence of 174 was generated randomly using Sealedenvelop.com. The participants were then distributed into one of the three study groups: Two intervention groups (virtual training and telephone training) and a control group. Figure 1 provides the CONSORT diagram.

CONSORT flow diagram
To conceal the random assignment list, a unique code was assigned to each group, known only to the principal investigator. To maintain blinding, the evaluator responsible for assessing the study outcomes remained unaware of the intervention types. The questionnaires for all groups were coded, and the final evaluator remained blinded to group assignments. Additionally, the data was submitted to a statistician for blinded analysis using the randomization code.
All eligible women were initially invited to participate via phone using the Iranian integrated electronic health system (SIB system). Contact continued with eligible women in each comprehensive center until the required number of samples was achieved. The study’s purpose and procedures were explained, and if participants expressed interest, the consent form was completed during the phone call, in the presence of a healthcare provider.
Baseline questionnaires were administered through telephone interviews. Virtual training sessions were conducted using WhatsApp, where participants were randomly divided into 12 groups of 3 - 5 people. Each group attended four 60-minute classes over four weeks, including lectures and discussions. In the telephone training group, participants received the same training through two 15-minute calls per week for four weeks, with prearranged call days. Table 1 outlines the four educational topics. These topics were derived from authentic domestic sources and endorsed by university faculty (20-23). Participants in both groups were able to ask questions outside the scheduled training times.
| Subject | Values |
|---|---|
| First subject | We discussed the significance of children and childbearing in Islam, their benefits, and the societal, parental, and disadvantages of having a single child. |
| Second subject | We discussed the significant influence of important individuals in our lives, such as parents, spouses, in-laws, colleagues, friends, and healthcare professionals. Seeking their input can often provide valuable solutions, especially regarding decisions about having children. |
| Third subject | The discussion covered the facilities provided by society for having children and how individuals can manage the economic, financial, and educational challenges associated with parenting. |
| Fourth subject | The previous topics were reviewed, allowing participants additional chances to share their opinions. |
Educational Content from Various Sessions
Simultaneously with the intervention groups, a control group of 58 individuals was established on WhatsApp. To adhere to ethical guidelines, materials on general women's health, such as menstrual disorders, breast self-examination, Pap smears, and common female infections, were provided to the control group weekly. After the interventions, an educational brochure on childbearing was sent to all members of the control group.
3.2. Measurements
The data collection tool consisted of two parts:
(1) Demographic and fertility information form: This form included 16 questions covering age, occupation, education level, and the number of children in the family for both the woman and her husband. It also collected information on the age at marriage, the decision-maker regarding having children, and the history of abortion, stillbirth, child mortality, and their numbers.
(2) Attitude towards Fertility and Childbearing Scale (AFCS): Originally designed by Soderberg et al. in Sweden in 2013 (24), the Persian version of the scale was psychometrically validated by Baezzat et al. in Iran in 2017 through exploratory factor analysis and criterion validity methods (25). The Persian version contains 23 items and four subscales: "Child as a Pillar of Life," "Child as an Obstacle," "Postponing Fertility to the Future," and "Fertility Requires the Fulfillment of Prerequisites." The Cronbach's alpha coefficient for the entire questionnaire was 0.79, with individual subscale coefficients ranging from 0.73 to 0.85 (17). Responses were scored on a five-point Likert scale, ranging from one (completely disagree) to five (completely agree). A higher total score indicated a more positive attitude towards childbearing.
The Demographic and Fertility Information Form was administered before the intervention, while the attitude questionnaire was administered before, immediately after, and three months post-intervention.
3.3. Statistical Analysis
The analyzed data were processed using SPSS version 22 software. The Kolmogorov-Smirnov test was used to examine the normality of the data. For qualitative and quantitative analyses, Chi-square tests and analysis of variance (ANOVA) were applied, respectively. To address the study's concepts and assumptions, and to account for missing observations in the samples, a linear mixed model test was employed. This model allows for more flexible variance-covariance matrix structures, making it preferable to other methods as it does not impose restrictive assumptions on correlated structures. A P-value of less than 0.05 was considered statistically significant.
3.4. Ethical Considerations
This project was approved by the ethics committee of Babol University of Medical Sciences and the national ethics system with the code number IR.MUBABOL.REC.1399.166. Informed consent was obtained from all participants. All methods were carried out in accordance with relevant guidelines and regulations.
4. Results
A total of 174 eligible women were randomly assigned to three groups of 58 participants each. The mean age was 25.8 ± 3.4 in the telephone training group, 25.5 ± 5.3 in the virtual training group, and 26.6 ± 4.4 in the control group. Most participants were housewives with university degrees, and their husbands worked freelance. Additionally, the majority of participants across all groups had no history of miscarriage or stillbirth. There were no statistically significant differences in demographic and fertility characteristics among the three study groups prior to the intervention (Table 2).
| Variables | Telephone Training Group (n = 58) | Virtual Training Group (n = 58) | Control Group (n = 58) | P-Value |
|---|---|---|---|---|
| Wife | ||||
| Occupation | 0.981 | |||
| Homemaker | 41 (70.7) | 39 (67.2) | 42 (72.4) | |
| Home-based work | 4 (6.9) | 5 (8.6) | 4 (6.9) | |
| On-site work | 13 (22.4) | 14 (24.1) | 12 (20.7) | |
| Education | 0.351 | |||
| Elementary/middle school | 11 (18.9) | 4 (6.9) | 6 (19) | |
| High school | 19 (32.8) | 20 (34.5) | 19 (32.8) | |
| University degree | 28 (48.3) | 34 (58.6) | 33 (56.9) | |
| Siblings number | 0.349 | |||
| 1 - 2 | 16 (27.6) | 22 (37.9) | 21 (36.2) | |
| 3 | 22 (37.9) | 20 (34.5) | 18 (31) | |
| ≥ 4 | 20 (34.5) | 16 (27.6) | 19 (32.8) | |
| Husband | ||||
| Occupation | 0.554 | |||
| Business man | 37 (63.8) | 45 (77.6) | 42 (72.4) | |
| Employee | 10 (17.2) | 6 (10.3) | 7 (12.1) | |
| Manual Worker | 18 (18.9) | 7 (12.1) | 9 (15.5) | |
| Education | 0.282 | |||
| Elementary/middle school | 12 (20.7) | 4 (6.9) | 11 (19) | |
| High school | 21 (36.2) | 30 (51.7) | 20 (34.5) | |
| University degree | 25 (43.1) | 24 (41.4) | 27 (46.6) | |
| Siblings number | 0.878 | |||
| 1-2 | 10 (17.2) | 11 (19) | 11 (19) | |
| 3 | 19 (32.8) | 24 (41.4) | 17 (29.3) | |
| ≥ 4 | 29 (50) | 23 (39.7) | 30 (51.7) | |
| Decision to have children | 0.491 | |||
| Wife | - | 2 (3.4) | 2 (3.4) | |
| Husband | 5 (8.6) | 2 (3.4) | 3 (5.2) | |
| Both | 53 (91.4) | 54 (93.1) | 53 (91.4) | |
| Still birth history | 0.361 | |||
| No | 56 (96.6) | 57 (98.3) | 58 (100) | |
| Yes | 2 (3.4) | 1 (1.7) | - | |
| Abortion history | 0.843 | |||
| No | 50 (86.2) | 48 (82.8) | 48 (82.8) | |
| Yes | 8 (13.8) | 10 (17.2) | 10 (17.2) | |
| Wife's age | 25.8 ± 3.4 | 25.5 ± 5.3 | 26.6 ± 4.4 | 0.337 |
| Husband's age | 30.1 ± 9.3 | 29.9 ± 4.0 | 31.2 ± 6.3 | 0.167 |
| Marriage age of woman | 22.3 ± 2.4 | 21 ± 8.3 | 22.8 ± 7.4 | 0.101 |
Within-group analysis of variance revealed that the average scores for attitude and its subscales increased in both the telephone and virtual training groups immediately after the intervention and again three months later, compared to pre-intervention levels. This indicated an improvement in the attitude towards childbearing in both educational groups. However, the increase was statistically significant only three months after the intervention (Table 3).
| Variables | Telephone Training Group | Virtual Training Group | Control Group | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Before | After | Three Months Later | P-Value | Before | After | Three Months Later | P-Value | Before | After | Three Months Later | P-Value | |
| Overall attitude towards childbearing | 73.4 ± 14.2 | 76.1 ± 14.8 | 80.6 ± 11.7 | 0.000 | 72.1 ± 11.8 | 75.1 ± 14.0 | 78.5 ± 9.2 | 0.000 | 77.2 ± 12.5 | 76.8 ± 11.7 | 74.6 ± 10.9 | 0.023 |
| Attitude to the child as a pillar of life | 31.3 ± 5.2 | 32.6 ± 5.1 | 34.0 ± 4.3 | 0/000 | 31.0 ± 5.8 | 32.1 ± 6.6 | 33.0 ± 4.2 | 0.004 | 33.1 ± 5.1 | 33.2 ± 4.1 | 32.6 ± 4.4 | 0/392 |
| Viewing the child as an obstacle | 18.9 ± 6.3 | 19.8 ± 6.7 | 21.0 ± 4.8 | 0.000 | 18.3 ± 5.2 | 19.1 ± 5.7 | 20.5 ± 2.9 | 0.002 | 19.9 ± 5.3 | 19.0 ± 5.2 | 18.5 ± 4.6 | 0.004 |
| Postponing fertility to the future | 15.7 ± 4.1 | 16.9 ± 4.3 | 18.7 ± 3.9 | 0/021 | 15.8 ± 3.5 | 17.2 ± 4.1 | 18.3 ± 3.3 | 0.000 | 16.9 ± 4.3 | 17.4 ± 4.1 | 17.0 ± 3.8 | 0.326 |
| Fertility requires the fulfillment of prerequisites | 7.4 ± 2.0 | 6.7 ± 1.8 | 6.7 ± 1.2 | 0.000 | 6.8 ± 2.0 | 6.5 ± 2.1 | 6.5 ± 1.3 | 0.503 | 7.2 ± 2.3 | 7.0 ± 2.3 | 6.5 ± 1.5 | 0.153 |
The results of the linear mixed model test revealed a significant main effect of time on the scores of women's attitudes towards childbearing and its subscales (P < 0.05). The significance of time suggests notable changes in women's attitudes towards childbearing and its subscales over time, indicating that the training sessions contributed effectively to the increased scores. Additionally, the interaction effect of time and group on the scores of women's attitudes towards childbearing and its subscales (except for the subscale "Fertility Requires the Fulfillment of Prerequisites") was found to be significant (P < 0.05). This highlights a significant difference between the studied groups over time regarding the attitude towards childbearing and its subscales (Table 4).
| Variables | Group | Time | Group X Time | |||
|---|---|---|---|---|---|---|
| F Test | P-Value | F Test | P-Value | F Test | P-Value | |
| Overall attitude towards childbearing | 0.428 | 0.653 | 23.891 | < 0.001 | 14.868 | < 0.001 |
| Attitude to the child as a pillar of life | 0.034 | 0.967 | 15.288 | < 0.001 | 5.229 | < 0.001 |
| Viewing the child as an obstacle | 0.967 | 0.382 | 7.446 | < 0.001 | 8.854 | < 0.001 |
| Postponing fertility to the future | 0.357 | 0.700 | 38.949 | < 0.001 | 10.431 | < 0.001 |
| Fertility requires the fulfillment of prerequisites | 0.836 | 0.435 | 6.268 | < 0.001 | 0.531 | 0.713 |
Results of Assessing the Impact of Time, Group, and the Interaction Between Time and Group on Women's Attitudes Toward Childbearing and its Subscales a
5. Discussion
The current study compared the effectiveness of telephone and virtual training on women's attitudes toward childbearing. Results indicated a significant increase in the mean attitude scores towards childbearing in both the telephone and virtual training groups compared to the control group, three months post-intervention.
Maeda et al. conducted a study in Japan utilizing educational brochures on fertility knowledge provided by Airs software, which revealed enhanced fertility awareness and a shift in attitudes towards childbearing and its timing (26). Similarly, a 2018 controlled clinical trial with a two-year follow-up aimed at boosting fertility awareness and outcomes through online education showed significantly increased awareness in the intervention group, who also experienced quicker timing of new births compared to the control group (27). In Iran, a study improved fertility awareness and counseling skills among healthcare employees through face-to-face training and webinars, resulting in a significant increase in attitude scores (11, 19).
In the context of telephonic interventions, Zolfaghari et al. found that a three-month telephone intervention improved treatment adherence and glycosylated hemoglobin levels in patients with type 2 diabetes (28), findings which align with those of Samimi et al. (29). Similarly, telephone counseling was shown to enhance knowledge and performance related to COVID-19, while reducing anxiety (30). However, not all studies demonstrated positive effects. For instance, Cote and Gagne explored the impact of a structured educational intervention on clinicians' attitudes toward evidence-based programs (EBPs) in reproductive health but found no significant changes in attitudes or improvements in program implementation outcomes (31). Jalambadani et al. also found no impact of an educational intervention based on the theory of planned behavior on menopausal women's mental norms regarding sexual performance (32). These varying results can be attributed to differences in intervention design, participant demographics, and methodological approaches. Tailoring educational content to specific cultural and individual needs, as well as using robust and engaging delivery methods, significantly impacts the effectiveness of such interventions (32).
Attitude is a key factor in determining behavioral intention and performance (33). According to Rocklage and Fazio, attitude involves feelings, desires, and thoughts that drive behavior (34). In reproductive health, empowering women and fostering positive attitudes is crucial for influencing reproductive choices and decisions. A positive attitude towards parenthood often requires preparation for the responsibilities and challenges of raising children. Conversely, a negative or fearful attitude may prompt individuals or couples to postpone or reconsider the decision to have children. Understanding and addressing attitudes towards parenting are essential for making informed and comprehensive choices. A positive and informed attitude towards having children fosters a supportive and nurturing family environment, significantly impacting the well-being of both parents and children (35).
Previous research underscores the critical role of education in shifting negative attitudes towards childbearing (24). When individuals view children as valuable and perceive interactions with them as pleasurable rather than burdensome, they are more likely to choose parenthood. Education plays a pivotal role in reshaping these views and fostering positive attitudes. Tailoring educational methods to fit specific contexts, cultural backgrounds, and learning preferences enhances effectiveness and ensures meaningful attitude changes. By customizing teaching strategies, educators can create a more engaging learning experience that promotes positive attitudes and leads to substantial transformation (35).
The study faced limitations such as slow internet speeds and occasional disconnections, as well as the challenge of ensuring blinding based on the type of intervention. Additionally, the results may not be generalizable to rural women due to differences in cultural attitudes toward having children. Therefore, caution should be exercised when applying these findings more broadly. However, a key strength of this study lies in its unique approach, comparing two educational methods across different groups. This contrasts with most studies that typically focus on a single or blended learning method. The comparative design provides a more comprehensive understanding of the effectiveness of various educational approaches, which could have broader implications for public health policy and future research.
This study also opens avenues for further investigation, particularly in addressing its limitations and enhancing the generalizability of its findings. By comparing average attitude scores with other studies, this research offers valuable insights into the role of education in shaping women's attitudes toward childbearing. These insights are important for developing more effective educational programs tailored to specific populations, ultimately fostering positive attitudes and behaviors related to childbearing and family planning.
5.1. Conclusions
Both telephone and virtual training demonstrated a lasting positive impact on women's attitudes toward childbearing. Given the significance of favorable attitudes in influencing the demographic future of a country, implementing distance education programs, including mobile-based and internet-based approaches, offers an effective solution. These programs have the potential to increase awareness and foster positive attitudes toward childbearing. The accessibility and affordability of these methods further emphasize their role as a viable platform for promoting positive societal perspectives on childbearing.
