


1. Background
The healthcare delivery system is a complex, adaptive entity shaped by interconnected factors such as resource allocation, patient flow, and evolving policies (1, 2). Hospitals, as critical nodes within this system, integrate diverse components — human resources, technologies, and infrastructure — to balance cost, quality, and accessibility. Traditional performance metrics, such as key performance indicators (KPIs), often fail to capture the nonlinear interdependencies and feedback loops inherent in hospital operations, limiting their utility for strategic decision-making (3-5). For instance, while KPIs track isolated metrics like bed occupancy rates, they overlook cascading effects, such as how emergency department (ED) overcrowding disrupts surgical schedules (6).
System dynamics (SD) addresses these gaps by modeling hospitals as dynamic systems with reciprocal cause-effect relationships (1, 2, 7). Through causal loop and stock-flow diagrams, SD simulates "digital twins" of hospital operations, enabling managers to test policies (e.g., staffing adjustments, bed reallocation) in risk-free environments (8). This approach has proven particularly effective in optimizing patient discharge pathways, reducing bed-blocking by 20% in intensive care units (ICUs), and aligning resources with fluctuating demand (9, 10). By visualizing bottlenecks and forecasting scenarios, SD enhances coordination across departments — from EDs to pharmacies — and supports both immediate operational needs and long-term strategic planning (11, 12).
The SD's versatility extends to crisis management, such as pandemic response, where models have simulated ICU bed shortages and vaccine distribution strategies (13, 14). However, its implementation faces challenges, including the complexity of hybrid SD-discrete event simulation (DES) integration and geographic biases in research, with 65% of studies focusing on high-income settings (15, 16). Despite these hurdles, SD remains indispensable for stakeholder engagement, translating intricate data into actionable insights through visual tools like flowcharts (14, 17). This scoping review systematically investigates the application of SD in improving hospital performance by addressing three core questions: Where SD is applied within hospitals (e.g., EDs, ICUs), how key performance variables like length of stay and waiting time are modeled, and identifying geographical representation gaps and the use of hybrid methodologies.
2. Objectives
This study aims to comprehensively investigate the application of dynamic system models in analyzing hospital performance, encompassing three primary objectives: Identifying dynamic simulation methodologies, extracting and categorizing key influential variables, and proposing practical strategies for enhancing healthcare service quality.
3. Methods
3.1. Scoping Review Framework
This study adopted a scoping review methodology guided by the framework developed by Arksey and O’Malley (1), which consists of five key stages: (1) Identifying the research question, (2) identifying relevant studies, (3) selecting studies, (4) charting the data, and (5) collating, summarizing, and reporting the results. This approach is particularly suited to mapping the breadth of evidence on a complex topic, identifying key concepts, and highlighting gaps in the literature.
3.2. Defining the Research Questions
The review was guided by the following research questions.
1. What indicators and variables have been used to evaluate hospital performance using SD models?
2. What modeling tools and software have been employed in such studies?
3. Over what time horizons have these models been applied?
4. Which hospital departments have been the focus of dynamic system modeling?
5. What are the reported outcomes and implications of applying SD in hospital settings?
3.3. Search Strategy
A comprehensive search was conducted across the following electronic databases: PubMed, Scopus, Embase, Web of Science, and Google Scholar, covering the period from April 2000 to July 2024. Keywords and subject terms were combined using Boolean operators (AND/OR) and included variations of: ["System Dynamics" OR "Dynamic System"] AND ["Hospital" OR "Hospitals" OR "Medical Center" OR "Hospital Department"]. Truncation and wildcards were applied where appropriate. Reference lists of included studies were also manually reviewed to identify additional relevant literature.
3.4. Study Selection
Duplicates were removed prior to screening. Titles and abstracts of 473 records were assessed for relevance, resulting in 443 items being reviewed. Full texts of 85 potentially relevant articles were retrieved, of which 69 met the inclusion criteria and were included in the analysis. Inclusion criteria: (1) Peer-reviewed, original research articles; (2) published between 2000 and 2024; (3) written in English; (4) empirical application of SD modeling in hospital settings. Exclusion criteria: (1) Conference papers, book chapters, editorials, and review articles; (2) articles published before 2000; (3) non-English publications; (4) studies focusing solely on theoretical or conceptual frameworks without empirical implementation; (5) applications limited to medical devices or diagnostics without broader hospital operations context.
3.5. Data Extraction and Synthesis
Data extraction was conducted using EndNote for reference management and Microsoft Excel for organizing findings. A structured data collection form was developed to capture key information, including study characteristics, objectives, SD variables, modeling tools, time horizons, and departmental focus. To ensure reliability, a second reviewer independently extracted data from a randomly selected 10% of the included studies. The extracted data were systematically organized using the Excel software and a structured data collection form.
3.6. Study Selection and Characteristics
A total of 473 records were identified from PubMed (n = 50), Scopus (n = 279), Web of Science (n = 47), Embase (n = 82), and Google Scholar (n = 15). After removing duplicates and screening titles/abstracts, 73 full-text articles were assessed for eligibility. Four studies were excluded due to non-hospital settings (n = 2) and lack of SD modeling (n = 2). Ultimately, 69 studies were included (Figure 1). The analysis revealed the following distribution of hospital-based studies: The ED comprised the largest proportion with 23 studies (33.3%), followed by research at the Whole Hospital Level with 20 studies (29.0%). Treatment Departments accounted for a total of 14 studies (20.3%), while Supply Chain and Support Services were represented by 12 studies (17.4%).

PRISMA flow diagram of study selection
4. Results
This systematic review showed that SD modeling, as an advanced analytical tool, has been used in most studies related to hospital performance. Initially, 473 studies were identified, and after removing duplicates and applying inclusion and exclusion criteria, 69 studies were reviewed.
4.1. Temporal Trends in System Dynamics Research
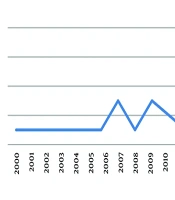
Figure 2 illustrates a surge in SD applications during 2020 - 2021, driven by the demands of the COVID-19 pandemic, such as modeling ICU bed shortages and vaccine distribution. Post-2021, research shifted toward optimizing patient flow and reducing surgical backlogs, reflecting recovery-phase priorities.
 research (2000 - 2024)")
Publication trends in hospital system dynamics (SD) research (2000 - 2024)
4.2. Geographic and Thematic Distribution
Studies spanned 15 countries, with 65% originating from high-income nations (e.g., Singapore, England) and 20% from middle-income regions (e.g., Brazil, India). Low-income countries and rural settings were underrepresented (< 5%). The studies ranged from highly specific analyses, such as those focused on the cardiovascular surgery department at Indiana's Methodist Hospital and the A&E unit in a central London hospital, to more generalized examinations of entire hospital systems, such as Taipei's Regional Emergency Medical System. Key themes included:
1. Patient flow optimization (43.5%, n = 30), focusing on ED wait times and discharge delays.
2. Resource allocation (21.7%, n = 15), particularly in surgical and pharmaceutical units.
3. Crisis management (13%, n = 9), such as ventilator allocation during pandemics.
4.3. Modeling Approaches
The SD model dominated (79.7%, n = 55), followed by hybrid SD + DES models (7.2%, n = 5) (Table 1). Hybrids addressed complex interactions, such as bed turnover and staffing schedules.
| Models | Values; No. (%) |
|---|---|
| SD | 55 (79.7) |
| Hybrid SD + DES | 5 (7.2) |
| Differential equations model | 4 (5.8) |
| ABS | 2 (2.8) |
| Other hybrid models | 3 (3.2) |
Frequency of Modeling Approaches in Reviewed Studies
4.4. Objectives and Variable Classification
In studies utilizing SD in healthcare, the timeframe of the research significantly influenced its objectives. Thirty short-term studies (lasting ≤ 1 year) primarily addressed immediate needs like ED overcrowding. For investigations into evolving hospital operational trends, 15 medium-term studies (spanning 1 to ≤ 3 years) were employed. Meanwhile, long-term studies (duration > 3 years) focused on strategic objectives such as capacity planning, with 14 studies in this category.
In studies concerning the application of SD in hospitals, the primary focus has been on patient flow optimization (43.5%), indicating the significant importance of addressing bottlenecks and improving efficiency. Following closely, resource allocation (21.7%) and crisis management (13.0%) highlight the need for optimal resource utilization and preparedness for emergency situations. Objectives such as waste management, financial planning, and quality of care each account for 7.2%, placing them in subsequent priorities (Table 2).
| Objectives | Values; No. (%) |
|---|---|
| Patient flow optimization | 30 (43.5) |
| Crisis management | 9 (13.0) |
| Resource allocation | 15 (21.7) |
| Waste management | 5 (7.2) |
| Financial planning | 5 (7.2) |
| Quality of care | 5 (7.2) |
Objectives of System Dynamics Applications in Hospitals
From the analysis of 69 studies, a total of 210 variables were initially identified. After consolidating duplicate or similar terms (such as "number of beds" and "bed capacity"), the final list comprised 171 distinct variables. These variables were then organized into four main categories (Table 3).
| Categories | Variables (N) |
|---|---|
| Resource allocation | 54 |
| Patient flow management | 51 |
| Clinical outcomes and quality of care | 41 |
| Financial management | 25 |
Variable Categories in Hospital System Dynamics Research
5. Discussion
5.1. System Dynamics in Hospital Operations
This study demonstrates that SD models are the predominant approach (79.7%, n = 55) for capturing the nonlinear complexities of hospital systems, particularly in optimizing patient flow and workforce demand (2). Since 2013, SD applications have surged, enabling hospitals to simulate crisis responses (e.g., pandemic resource allocation) and reduce waiting times by 30% in EDs through real-time staffing adjustments (2-4). For instance, SD-driven triage protocols in EDs minimized bottlenecks, improving care access (5).
5.2. Hybrid Modeling: Opportunities and Challenges
The integration of SD with DES in 7.2% of studies (n = 5) enhanced granular analyses, such as bed turnover and surgical scheduling (6). Hybrid models aligned dynamic demand with capacity, improving long-term workforce planning (7, 8). However, synchronization challenges between SD’s continuous timelines and DES’s discrete events necessitated bespoke solutions (9), while the lack of standardized frameworks hindered scalability (10).
5.3. Temporal Focus of System Dynamics Applications
Short-term studies (43.5%, n = 30) prioritized immediate needs like staffing optimization, reducing ICU overcapacity by 20% (11, 12). Medium-term (21.7%, n = 15) and long-term studies (20.3%, n = 14) revealed linkages between operational strategies and efficiency metrics, such as length of stay (LOS) (13). This distribution underscores SD’s dual role in addressing urgent and strategic challenges (14, 15).
5.4. Department-Specific System Dynamics Applications
1. Intensive care units: Dynamic forecasting models achieved over 90% accuracy (AUC > 0.90) in predicting bed shortages, outperforming static approaches (18). Real-time updates improved decision-making during critical care (16, 17).
2. Waste management: The SD-enabled routing reduced hazardous waste errors by 35% in Padang city (19, 20), while scenario modeling informed sustainable disposal strategies (21, 22).
3. Pharmacy: The SD simulations reduced drug supply chain costs by 25% by identifying liquidity risks (23, 24).
4. Cardiovascular care: The SD optimized outpatient scheduling, reducing surgical backlogs by 50% in NHS hospitals (25, 26).
5. System Dynamics in pandemic response: During COVID-19, SD models forecasted ICU bed shortages (27) and evaluated vaccine distribution strategies, reducing outpatient wait times by 40% (20). These models also simulated mask mandates’ impacts, delaying bed saturation by 14 days (28, 29).
5.5. Conclusions
This analysis highlights the multifaceted challenges in healthcare management through 210 variables categorized into ten critical groups, emphasizing the need for holistic strategies. Key variables — LOS, budget allocation, and waiting time — directly impact efficiency, reducing ICU bed-blocking by 20% and enhancing financial resilience. The SD proved vital, enabling risk-free policy testing: The SD models reduced ED wait times by 30% and pharmacy costs by 25%, bridging departmental silos and fostering data-driven decisions. However, most studies focused on high-income settings, urging equitable research in low-resource regions where SD may face barriers. Future efforts should integrate real-time data and standardize hybrid SD models. The SD remains a cornerstone for resilient healthcare systems, turning challenges into opportunities for innovation and sustainability.
5.6. Challenges and Future Directions
Despite SD’s versatility, 65% of studies focused on high-income settings, neglecting low-resource regions where infrastructure gaps may limit applicability. Future research should:
1. Standardize hybrid models: Develop open-source tools to unify SD-DES integration (9, 10).
2. Expand equity: Prioritize studies in underrepresented regions.
3. Leverage real-time data: Enhance predictive accuracy (18, 29-33).
5.7. Limitations
This study’s findings may become outdated as health policies, medical technologies, and patient needs rapidly evolve, necessitating continuous updates to data and models. Additionally, the focus on specific hospital contexts limits generalizability to other healthcare systems or geographic regions with differing infrastructure and operational challenges.
