1. Introduction
The trophic ulcer is one of the leprosy sequelae due to peripheral neuropathy (1). The pathogenesis is mainly related to the abnormally increased pressure in areas such as the sole, secondary to the lack of sensation, and deformities induced by peripheral sensory-motor neuropathy (2). Trophic ulcers can cause economic and social burdens, and may influence the patient’s quality of life (2, 3). Trophic ulcer in leprosy patients can pose a significant stigma to the patients and remain challenging to clinicians due to the low response to treatment (3).
Recent studies have reported the effectiveness of Platelet-rich plasma (PRP) in the management of chronic ulcers. Platelet-rich plasma contains growth factors to increase the proliferation of mesenchymal stem cells, osteoblasts, fibroblasts, endothelial cells, and epidermal cells, thereby stimulating tissue regeneration, new blood vessel vascularization, and reepithelialization, which are beneficial in the process of wound healing (2). We report a non-healing trophic ulcer in a leprosy patient treated with a combination of injection and topical PRP.
2. Case Presentation
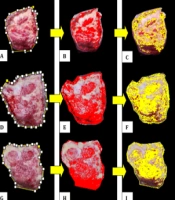
A 61-year-old female patient referred to complaining of a non-healing wound in her right foot since two months ago. The wound was becoming larger, but not painful and without pus or bleeding condition. She treated the wound with sodium chloride compress and gentamycin ointment without any improvement. She was a leprosy patient with already finished medication since 19 years ago. She had another wound on the right toe a year ago. She denied a history of diabetes mellitus and hypertension. The general status was in normal condition. A skin examination on the right plantar pedis showed a solitary ulcer sized 1 × 0.5 × 0.3 cm and a linear ulcer sized 2.5 × 3 × 0.3 cm with callus in the surrounding (Figure 1). The sensoric test with SWM showed decreased sensory in the magenta monofilament (300 g). The whole blood test, blood glucose (96 mg/dL), renal function, and kidney function showed no abnormality. Gram examination from the base of the ulcer showed no bacteria. We diagnosed a trophic ulcer and treated it with a combination of injection and topical PRP every week.

Figure 1.
Trophic ulcer before PRP treatment
Platelet-rich plasma was made by taking 8 cc of blood from the patient’s cubital vein. Blood samples were centrifuged at 2,150 rpm for 3 min. The serum was transferred into a sterile tube and centrifuged again at 4,000 rpm for 6 min. Platelet-rich plasma was applied after ulcer cleaning with a betadine solution and debridement of the callus around the ulcer. The injection of 0.1 mL subcutaneous PRP was applied with a 1 cm distance from the site of the previous injection. Platelet-rich plasma was also applied topically on the ulcer. After procedural, the ulcer was closed with sterile gauze and plaster until the next PRP treatment. The clinical result showed that the ulcer completely healed in four weeks of PRP treatment (Figure 2) and no side effect appeared during treatment.

Figure 2.
Trophic ulcer after PRP treatment
3. Discussion
The trophic ulcer is a common sequela of grade II disability in leprosy patients. Chavan and Patel (4) reported 61.5% of leprosy patients with trophic ulcers. The characteristic of trophic ulcers is the callus formation around the ulcer, accompanied by anesthesia. The predilection of trophic ulcers in leprosy patients is on the forefoot and big toe (79%), midfoot (7%), or hindfoot (14%) (1, 5). The pathogenesis of trophic ulcers in leprosy patients is due to dynamic and/or static deformity on the numbness skin to constant high pressure (1, 3).
There are various therapeutic modalities for trophic ulcers, including debridement, wound care, wound-dressing, topical antibiotics, application of growth factors, Negative pressure wound therapy (NPWT), and reconstructive surgery. The management of trophic ulcers should be based on the pathogenesis of these ulcers (1). Recent studies have reported the effectiveness of PRP in the management of chronic ulcers.
Platelet-rich plasma is a plasma-derived product of autologous blood, which has higher than normal platelet concentration (2). Platelet-rich plasma contains activated autologous growth factors and releases several growth factors, chemokines, and cytokines, including Platelet-derived Growth Factor (PDGF), Vascular Endothelial Growth Factor (VEGF), Epidermal Growth Factor (EGF), Fibroblast Growth Factor (FGF), Transforming Growth Factor (TGF)-β, Insulin-like Growth Factor (IGF), Interleukin (IL)-8, Macrophage Inflammatory Protein (MIP)-1α, and Platelet Factor (PF) 4 (6, 7). In PRP, activated platelets also release numerous other compounds such as fibronectin, vitronectin, and sphingosine 1-phosphate, which are essential in wound healing (8).
Crovetti et al. reported the effectiveness of topical PRP in the gel form in 24 cases of chronic ulcers with various causes such as diabetes mellitus, trauma, neuropathy, vascular insufficiency, and vasculitis. The result of the study showed that nine patients experienced complete reepithelialization and the rest experienced reduced wound size of more than 50% compared to before treatment (9). Carter et al. reported that the application of PRP on ulcers showed faster healing response and lower pain and infection than conventional therapy (10). A study by Anandan et al. on 50 leprosy ulcer patients showed 92% complete healing after six times of topical PRP application (3). Conde-Montero et al. reported two cases of recalcitrant chronic ulcers in leprosy patients that showed complete reepithelization after nine weeks of PRP injection (2). Side effects that can occur in PRP therapy include infection, discoloration of the skin, bruising, pain in the injection area, emboli following PRP injection, and allergic reactions (very rare). Clinicians still have to be careful of allergic history because activated platelets also release histamine (7). We managed our case with a combination of injection and topical PRP with a one-week interval. The clinical result showed that the ulcer completely healed in four weeks of PRP treatment and no side effect appeared during treatment.
3.1. Conclusions
Trophic ulcers in leprosy patients pose a significant stigma to the patients and remain challenging to clinicians due to the low response of treatment. A combination of injection and topical PRP showed to be promising in the management of non-healing trophic ulcers in leprosy patients.