


1. Background
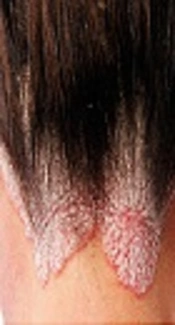
Psoriasis is one of the most common chronic skin diseases around the world, with a prevalence of 1.4% to 2.9%. The scalp is one the most common sites of Psoriasis. Symtoms include scaly red patches, Silvery-white Dry scalp, itchiness, burning or hair loss. Different topical drugs are used for psoriasis treatment, such as coal tar, vitamin D3 analogues, and corticosteroids (1-3). Calcipotriol as a vitamin D3 analogue has been used to treat psoriasis since 1991. It is documented that calcipotriol ointment is at least as effective as betamethasone (1, 2). Adverse events of calcipotriol are mild and its safety has been shown by many studies (3, 4) and topical corticosteroids are extremely useful for treatment of scalp psoriasis. Betamethasone dipropionate is classified as a potent steroid group and is prescribed topically to treat scalp psoriasis on a short-term duration.
Calcipotriol and corticosteroids act in different mechanisms (4, 5) thus higher efficacy may be achieved by their combination. Calcipotriol as a vitamin D3 analogue binds to the vitamin D receptor, which works as a heterodimer with the retinoid receptor RXR. Vitamin D analogues reduce epidermal hyperproliferation and abnormal keratinization, induce apoptosis in lymphocytes, inhibit production of Th1 cytokines, and habe an anti-angiogenic effect (6, 7). Corticosteroids bind to glucocorticoid receptors in the cytoplasm and transduce signals to the nucleus in order to stimulate or inhibit genes, which are responsible for inflammation (8). Corticosteroids decrease mediators of inflammation (e.g. prostaglandins, leukotrienes, etc.) and inhibit production and release of different cytokines (e.g. interleukin (IL)-1, IL-8, and different interferons, like IFNγ) (9-11). Combination of calcipotriol and betamethasone is more efficient than monotherapy and also different studies have shown its effect in decreasing proliferation of keratinocytes during at least a 4-week treatment duration. The purpose of this study was to compare the effects and side effects of combination treatment with its effective components prescribed alone in the Iranian population.
2. Methods
Patients aged 18 years or above with a clinical diagnosis of scalp psoriasis that had 10% or more scalp involvement with clinical signs, such as erythema, scaling, and moderate thickness, were recruited. They did not need systemic therapy and also patients, who had used systemic anti-psoriatic treatment within the previous 4 weeks or topical treatment on their scalp (expect emollient and therapeutic shampoos), were excluded. Other exclusion criteria included the use of biologic agents for the previous 6 months, scalp atrophy, current diagnosis of pustular or erythrodermic psoriasis, scalp infection with bacteria, fungi or parasites, abnormality in calcium metabolism with severe renal failure or clinical signs of hypercalcemia, and severe liver dysfunction. Patients (n = 54) were randomized to two groups and received up to 8 weeks of treatment. The groups included:
Combination group: calcipotriol ointment once daily plus betamethasone lotion once daily (at night).
Control group: betamethasone lotion twice daily.
The extent and severity of scalp psoriasis were recorded at each visit (week 2, 4, 6, and 8). The severity of the lesions was categorized to 6 scores by investigator’s global assessment (IGA) scale (12). Sum of signs (redness/erythema, scale/crusting, and thickening/elevation) and symptoms (pruritus) using a 3-point scale (e.g. 0 = none, some = 1, and extensive = 2) was used as a criterion for severity. Scores varied from 0 to 12. Each level of severity (clear, mild, and moderate) was defined in a standardized fashion as total severity sign (TSS) score for psoriasis (13). Patient’s global assessment (PGA) was used for patient’s satisfaction (13). Prior to entrance of patients, independent ethics committees approved the study and patients signed an informed consent.
The SPSS 16 (SPSS Inc.CHICAGO, IL, USA) statistical software was used for data analysis. P values of less than 0.05 were considered statistically significant. Categorical data are summarized as numbers (percentages). The chi-square test was used to test the differences of frequency distributions in contingency tables. The independent-samples t-test compared the dependent variable between the two groups. The repeated measures ANOVA was used to compare means of the variables.
3. Results
Fifty-four eligible patients with scalp psoriasis were randomly allocated to two groups. The baseline demographic and clinical characteristics of participants are summarized in Table 1. At the end of the study, 27 patients in the bethametasone and calcipotriol group and 23 patients in the bethametasone group as monotherapy attended the pre-determined visit (visit of week 2, 4, and 8) after the baseline visit. Periocular dermatitis and pustule in scalp was reported in 4 patients in the bethametason group and they were excluded from the study. None of the patients in the case group developed any complication. The two groups did not differ significantly in gender and age. The efficacy endpoint was indicated by the proportion of subjects with “absence of disease” or “very mild” disease according to IGA score (P value: 0.04), cleared disease was based on the PGA score (P value: 0.005), and Tss ≤ 1(P value: 0.031) at week 2, 4 and 8 (Table 2).
| Variables | Combination Group Therapy (N = 27) | Bethametasone Therapy (N = 23) |
|---|---|---|
| Age, y, mean ± SD | 35 ± 10.6 | 42.2 ± 7.7 |
| Gender | ||
| Male | 15 (50) | 15 (50) |
| Female | 12 (60) | 8 (40) |
| Disease duration | 7.4 ± 3.5 | 9.6 ± 3.9 |
| IGA score (baseline) | ||
| Absence of disease | 0 | 0 |
| Very mild | 0 | 0 |
| Mild | 3 (11) | 3 (13) |
| Moderate | 11 (41) | 10 (43) |
| Severe | 7 (26) | 7 (31) |
| Very severe | 6 (22) | 3 (13) |
| Tss score(Baseline) | 7.6 ± 2.4 | 6.9 ± 2.2 |
Baseline Demographics and Clinical Characteristics of the Study Groupa
| Variables | Week 2 | Week 4 | Week 8 | P Value |
|---|---|---|---|---|
| IGA score | ||||
| Calcipotriol group | 4 (15) | 13 (48) | 17 (63) | 0.04 |
| Control group | 0 | 2 (9) | 0 | |
| PGA score | ||||
| Calcipotriol group | 2 (7) | 9 (39) | 17 (63) | 0.007 |
| Control group | 0 | 0 | 10 (37) | |
| TSS score | ||||
| Calcipotriol group | 5.1 ± 2.5 | 3.2 ± 2.1 | 1.7 ± 1.6 | 0.004 |
| Control group | 5.4 ± 2.2 | 4.6 ± 1.9 | 3.1 ± 1.6 |
IGA, PSA, TSS Score Over Time Between the Two Study Groupsa
The mean TSS score of both groups was reduced continuously from baseline to week 8 of study (Table 2). The case group in comparison with the control group had an additional 3 points decrease in the mean TSS score (P value: 0.004). Based on IGA and PGA score, scalp psoriasis had greater improvement in the case group compared to the control group, respectively (P value: 0.04, P value: 0.007). Mean duration of treatment in the combination group was about 5 weeks and in the monotherapy, this was about 7 weeks (P value: 0.002).
4. Discussion
Many studies have been designed to treat scalp psoriasis due to its high prevalence. Since the etiology of this disease is not clearly known, there is no definite therapy for it. On the basis of histopathology results of previous studies, immune system dysregulation and inflammatory processes have been demonstrated to have great roles in scalp psoriasis. Most medications of psoriasis are immune modulators like vitamin D3 synthetic analogues and corticosteroids. In this study, result and quality of treatment was assessed by 3 criteria, such as TSS, PGA, and IGA. The primary objective of this study was to compare the clinical efficacy and evaluate the mentioned criteria in calcipotriol/betamethasone (the combination) treatment with betamethasone dipropionate treatment alone in patients with scalp psoriasis after 8 weeks. An 8-week treatment regimen was chosen to verify the primary response to therapy, the degree, and duration of treatment. Previous studies (14, 15) showed that combination therapy may provide a shorter time treatment plan. However, the aim of this study was not intended to determine the duration of treatment. The mean decrease in TSS at the end of the study was significantly greater in the combination group (about 6) compared to betamethasone alone (about 3). The results from the present study are in agreement with previous studies, which have shown that the combination therapy is superior in efficacy to monotherapy (16, 17). In addition, this is the first study that estimates the efficacy of combination therapy in scalp psoriasis in Iran. Data from other measurements of efficacy (speed of response, change in IGA, and PGA) also showed statistical differences between the two groups. From the clinical point of view, 63% of participants in the combination therapy group achieved the goal of treatment; this was only seen in 35% of the monotherapy group. Furthermore, the convenience of patient to use combination therapy was more than applying one drug twice daily. On the other hand, the mean decrease in TSS in patients of the combination group after 4 weeks was statistically significant (approximately 4) compared to the monotherapy group (approximately 2). Using combination therapy will reduce steroid-related adverse events. Potent topical corticosteroid preparations used for long periods or in excessive quantities may lead to skin atrophy as a well-recognized dermatological risk (18-20). Corticosteroid-induced skin atrophy is a consequence of collagen synthesis inhibition in connective tissue (18). Using low potency corticosteroids or their application in short periods of time may reduce the chance of permanent atrophy (17, 21). Surprisingly, as opposed to the skin-thinning effects of betamethasone, calcipotriol alone has been shown to cause skin thickening, thus skin atrophy would not be expected to occur with its use in combination with betamethasone (18, 21). The overall proportion of patients reporting lesional/perilesional adverse reactions to the combined formulation was significantly less than the betamethasone group. Periocular dermatitis in monotherapy was reported by 3 patients and pustule in scalp by 1 patient but none of the patients in the combination group reported the mentioned complications. These results support data from other studies (18), which demonstrated that the risk-benefit ratio for the combination therapy is favorable over monotherapy. Future studies are needed to evaluate the long-term safety potential of the combination therapy for scalp psoriasis.
4.1. Conclusion
The results of the present study revealed that combinatorial treatment of psoriasis with calcipotriol and betamethasone is a reliable and low-complication method compared with the single-drug betamethasone regimen and has better treatment efficacy.
