Fulltext
Full Text Available is PDF
Authors
Cardiac fungal infections have become more prevalent and are being diagnosed with increasing frequency. The most common infective organism is Candida albicans, followed by Aspergillus fumigatus and Cryptococcus. Cardiac involvement is usually associated with endocarditis, myocarditis, pericarditis, or intracardiac fungal mass. Early diagnosis is imperative, as these patients have poor outcome once there is cardiac involvement(1).
Cardiac tumors are diverse in clinical presentation but several clinical features including embolisation, obstruction and arrhythmias are seen commonly with many cardiac massesA four month old male infant, with a history of low birth weight and several admissions at different hospitals who had a history of femoral and umbilical catheterization referred to our center.
On examination there was mild cyanosis, normal heart sounds with 2/6 systolic murmur at LSB. Lungs were clear.
Laboratory data showed a normochromic normocytic anemia with other hematologic parameters in the normal range. Blood culture was positive for candida albicans. Chest X-ray was unremarkable.
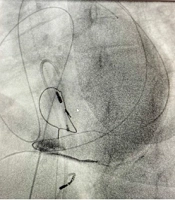
Echocardiography revealed a large pedunculated RA mass. (Figure 1). Besides, there were a perimembranous VSD ( ventricular septal defect), 0.53 cm in diameter and a medium size PDA (patent ductus arteriosus) with subsystemic pulmonary hypertension and global ejection fraction in the ranger of 80%.
In the operating room, under general anesthesia median sternotomy was performed. CPB established in usual manner using bicaval cannulation passingtape around them. After total bypass right atrium (RA) was opened and the mass (fungal vegetation) which had occupied most of the RA chamber and extended to the right ventricle was removed readily (Figure 2). Using the RA approach VSD, which was small, closed primarily with out using a patch. After re-warming and de-airing, the patient weaned from CPB easily. The CPB time and Aortic cross-clamp time was 53 and 25 minutes, respectively. The specimen is shown in Figure 7. ICU course was uneventful
© 2008, Multidisciplinary Cardiovascular Annals. This open-access article is available under the Creative Commons Attribution-NonCommercial 4.0 (CC BY-NC 4.0) International License (https://creativecommons.org/licenses/by-nc/4.0/), which allows for the copying and redistribution of the material only for noncommercial purposes, provided that the original work is properly cited.
Esmaeilzadeh M, Peighambari M, Parsaee M, Khamooshi A, Hosseini S. Fatal aortitis: a complication of aspergillus endocarditis following coronary artery bypass graft surgery. Int Cardiovasc Res J. 2018;1(3):e79526. doi:
Roodpeyma S. Infective Endocarditis Complicated by Septic Pulmonary Emboli in a Case of a Ventricular Septal Defect. J Compr Ped. 2015;6(4):e29610. doi: https://doi.org/10.17795/compreped-29610
Rastravan R, Azarfarin R, Babaei T, Tirgarfakheri K, Ghanbari M. Life Threatening Right Ventricle and Atrium Perforation and Tricuspid Valve Injury Due to Pacemaker Lead Dislodgment- A Case Report. Multidiscip Cardio Annal. 2022;13(1):e123135. doi: https://doi.org/10.5812/mca-123135
Shokohi T, Nouraei SM, Afsarian MH, Najafi N, Mehdipour S. Fungal Prosthetic Valve Endocarditis by Candida parapsilosis: A Case Report. Jundishapur J Microbiol. 2014;7(3):e9428. doi: https://doi.org/10.5812/jjm.9428
Mozaffari K. A One-year old infant with multiple cardiac masses and congenital heart disease (A case report). Multidiscip Cardio Annal. 2011;3(1):e8738. doi:
Last Update: 1 month ago
Last Update: 1 month ago
Last Update: 1 month ago
Last Update: 1 day ago