



1. Background
Dilated cardiomyopathy (DCM) is categorized by the presence of a dilated and poorly functioning left ventricle (LV) in the absence of abnormal loading conditions or coronary artery disease (1). Recently, a new category of DCM spectrum, hypokinetic non-dilated cardiomyopathy (HNDC), has been proposed by the European Society of Cardiology (ESC), defined by the combination of LV or biventricular global systolic dysfunction and normal LV size (1).
An apparent better evolution was hypothesized in the HNDC group compared to DCM patients (2-4).
The high prevalence of this early DCM phase in the general population and in DCM spectrum (2, 5), shows the importance of recognizing other aspects of this little-known entity, particularly echocardiographic parameters.
2. Objectives
We are considering the evaluation of right ventricular (RV) function in HNDC patients in this study.
3. Methods
HNDC patients defined as left ventricular ejection fraction (LVEF < 45%) without dilatation, not explained by abnormal loading conditions (i.e., history of severe hypertension, valvular heart disease or congenital heart disease) or coronary artery disease.
Normal LV size determined by LVEDVI ≤ 75 mL/m2 for men and LVEDVI ≤ 68 mL/m2 in women obtained from Iranian subpopulation according to the results of World Alliance of Societies of Echocardiography (WASE) Normal Values Study (6).
Finally, 31 HNDC patients who met the criteria and was referred to Shahid Rajaie Cardiovascular, Medical and Research Center (RCMRC) consecutively enrolled in the study from March 2018 to March 2019. Interviews were conducted to gather information on patients’ New York Heart Association (NYHA) classification, familial disease (with regard to ESC published criteria) (1), underlying disorders and heart medications. Moreover, data regarding prior imaging modalities such as CMR and coronary angiography were extracted from the patient’s electronic data sheets.
Two-dimensional (2-D) grayscale echocardiography was performed with Philips EPIQ7 ultrasound system for cardiology (Philips Ultrasound, Bothell, WA, USA) equipped with xMATRIX probe. The frame rate was > 50/s. Images were analyzed using Q-Lab, version 10 (Philips) by one single fellow of cardiology.
RV size was determined with 2-D measurement in the middle segment of the RV. RV function was evaluated by both 2D and Doppler tissue imaging. Tricuspid annular plane systolic excursion (TAPSE) measurement was performed from RV focused view by M-mode cursor position on the lateral tricuspid annulus. Quantification of RV function was also performed by RV fractional area change (RV FAC), calculating the percentage of RV area change between diastole and systole again from RV focused view (Figure 1).

FAC calculated by the percentage of the RV area change between diastole and systole. FAC, fractional area change; RV, right ventricular.
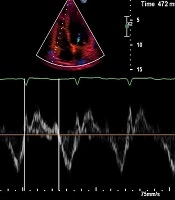
RV Myocardial performance index (MPI) derived from tissue Doppler method was calculated as (TCO - ET)/ET, where TCO is the time from tricuspid valve closure to tricuspid valve opening, and was measured as the time interval between the end of atrial systolic contraction (a’) of the preceding cardiac cycle and the beginning of early diastolic tricuspid valve annular velocity (e’) wave of the subsequent cardiac cycle that includes isovolumic contraction time, ejection time (ET) and isovolumic relaxation time (Figure 2). RV S’ velocity was also obtained from the tissue Doppler image as the highest positive systolic velocity while optimizing the gain to avoid noises.
We calculated the RV dysfunction score as described previously for chronic thromboembolic pulmonary hypertension (7) as the summation of points awarded for the presence of four parameters (TAPSE < 16 mm, 1 point; S’ < 10 cm/s, 1 point; RVFAC < 35%, 1 point; and RV-MPI > 0.55, 1 point) using the cut-off value recommended by ASE guidelines (8, 9).patients were divided into 5 groups based on their score: score 0 to 5. The higher the score, the worse the RV function.
/ET. ET, ejection time; MPI; myocardial performance index; RV, right venricular; TCO, tricuspid valve opening to closure time.")
RV tissue derived MPI calculated by using formula (TCO - ET)/ET. ET, ejection time; MPI; myocardial performance index; RV, right venricular; TCO, tricuspid valve opening to closure time.
Peak velocity of tricuspid regurgitation (TR) envelope achieved by continuous wave (CW) Doppler was used to calculate systolic pulmonary arterial pressure (SPAP) by applying the Bernoulli equation. The probability of pulmonary hypertension (PH) was graded according to ESC/ERS guidelines for the diagnosis and management of pulmonary hypertension (10).
Statistical analyses were performed using SPSS version 22 (IBM, Armonk, New York). One-sample Kolmogorov-Smirnov test was used to evaluate the normal distribution of the data. Categorical variables are presented as numbers and percentages. Continuous data are reported as median and interquartile range (IQR) or mean ± standard deviation. Categorical data were compared using chi-square test, and for continuous data, Mann-Whitney U test was run. The relationships were assessed using Pearson correlation coefficient (r) or Spearman rank correlation coefficient. P values of less than 0.05 were considered statistically significant.
4. Results
A total of 31 patients were enrolled in the study. The median age of the study population was 47 years (IQR, 33 - 57), 18 (58.1%) were men, and the median age of diagnosis was 43 years (IQR, 32 - 54). Among all study subjects 19.4% of patients reported a positive familial history. In addition, 19%, 54.8%, and 16.1% of the study group were in NYHA classification I, II, and III, respectively, while no patient stands in NYHA classification IV. Furthermore, most of the patients (90.3%) did not have a history of HF associated hospital admission. Nineteen patients (61.3%) had undergone CMR during the course of the disease (Table 1).
| Clinical Characteristics | HNDC (N = 31) |
|---|---|
| Male | 18 (58.1) |
| Age, y | 47 (33, 57) |
| Age of diagnosis, y | 43 (32, 54) |
| NYHA Class | |
| I | 9 (29.0) |
| II | 17 (54.8) |
| III | 5 (16.1) |
| IV | 0 (0.0) |
| Positive family history | 6 (19.4) |
| Heart medication | |
| β-blocker | 24 (77.4) |
| RAS blockade | 25 (80.0) |
| Loop diuretics | 9 (29.0) |
| Aldosterone receptor antagonists | 18 (58.1) |
| HF associated hospitalization | |
| 0 | 28 (90.3) |
| 1 | 2 (6.5) |
| 2 | 1 (3.2) |
| CMR | 19 (61.3) |
Abbreviations: BMI, body mass index; CMR, cardiac magnetic resonance imaging; HF, heart failure; NYHA Class, New York Heart Association classification; RAS blockade, renin-angiotensin system blockade.
aValues are expressed as median (P25, P75) or No. (%).
Echocardiographic characteristics were outlined in Table 2. The median LVEF was 40% (IQR, 35 - 42) and LVEDVI was 58.8 mL/m2 (IQR, 53 - 64). The median TAPSE, RV S’, RVMPI, and FAC were 18 mm (IQR, 15 - 21), 11.0 cm/s (IQR, 10.0 - 12.2), 0.57 (0.46 - 0.7), and 40% (33 - 45), respectively. Interestingly the probability of PH was interpreted as low in all study population with median SPAP 25 mmHg (IQR, 20 - 30). RV size was also within the normal range in all patients. The mean right ventricular ejection fraction (RVEF) obtained from CMR available in 19 patients was 44.9 ± 4.3%. The prevalence of RV dysfunction in HNDC patients is estimated 47.3% (9/19 patients) based on CMR-RVEF as the “gold standard” for RV function assessment while RVEF less than 45% was considered as low according to proposed reference ranges for CMR (11).
| Echocardiographic Parameters | HNDC |
|---|---|
| LVEF by 2D Simpson method, % | 40 (35, 42) |
| LVEDDI, cm/m2 | 2.7 (2.59, 2.9) |
| LVEDVI by 2D Simpson method, mL/m2 | 58.8 (53.0, 64.0) |
| SPAP, mmHg | 25.0 (20.0, 30.0) |
| RVMPI | 0.57 (0.46, 0.7) |
| TAPSE, mm | 18.0 (15.0, 21.0) |
| RV S’, cm/s | 11.0 (10.0, 12.2) |
| FAC, % | 40.0 (33.0, 45.0) |
| RVD, cm | 3.0 (2.6, 3.3) |
Abbreviations: FAC, fractional area change; LVEDDI, left ventricular end-diastolic diameter index; LVEF, left ventricular ejection fraction; LVEDVI, left ventricular end-diastolic volume index; RVD, right ventricular diameter; RVMPI, right ventricular myocardial performance index; RV S’, right ventricular peak systolic myocardial velocity; SPAP, systolic pulmonary arterial pressure; TAPSE, tricuspid annular plane systolic excursion.
aValues are expressed as median (P25, P7575) or No. (%).
Correlation assessment between the RV dysfunction score and CMR-RVEF depicted a strong negative linear correlation (r: -0.95) (On On the other hand, RVEF showed a significant difference between the five RV dysfunction score subgroups (P = 0.04), depicting the higher the RV dysfunction score, the lower the RVEF (Table 3).

Scatter plot of the RV dysfunction score and RVEF obtained from CMR. CMR, cardiac magnetic resonance imaging; RVEF, right ventricular ejection fraction.
| Overall | RV Dysfunction Score | ||||||
|---|---|---|---|---|---|---|---|
| N#19 | 0, N#6 | 1, N#4 | 2, N#4 | 3, N#2 | 4, N#3 | P Value | |
| RVEF, % | 44.9 ± 4.3 | 49.5 ± 1.5 | 47.0 ± 1.4 | 43.0 ± 1.1 | 41.5 ± 0.7 | 38.0 ± 1.0 | 0.04 |
Abbreviation: RVEF, right ventricular ejection fraction.
aValues are expressed as mean ± SD.
Table 4 shows the comparison of the RVEF between the four echocardiographic parameters: TAPSE (≥ 16 vs. < 16), S’ (≥ 10 vs. < 10), RVFAC (≥ 35 vs. < 35), and RVMPI (≥ 0.55 vs. < 0.55). Of note, three of four variables (RV S’, RVMPI, and FAC) showed a good correlation with RVEF while TAPSE failed to provide meaningful relationship with RVEF (P = 0.8).
| TAPSE | RV S’ | RVMPI | FAC | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| < 16 | ≥ 16 | P Value | < 10 | ≥ 10 | P Value | > 0.55 | ≤ 0.55 | P Value | < 35 | ≥ 35 | P Value | |
| RVEF | 45.1 ± 2.6 | 47.1 ± 3.1 | 0.8 | 38.7 ± 1.7 | 46.6 ± 3.2 | 0.02 | 42.7 ± 3.7 | 48.7 ± 2.8 | 0.03 | 41.0 ± 2.6 | 47.8 ± 2.9 | 0.05 |
Abbreviations: FAC, fractional area change; RVEF, right ventricular ejection fraction; RVMPI, right ventricular myocardial performance index; RV S’, right ventricular peak systolic myocardial velocity; TAPSE, tricuspid annular plane systolic excursion.
aValues are expressed as mean ± SD.
5. Discussion
RV dysfunction is implicated in poor clinical outcomes independently of the underlying mechanism of disease. RV dysfunction is more prominent in subjects with more advanced left sided HF. In this setting, various pathogenesis may interfere in RV dysfunction including increased RV afterload from postcapillary PH, volume overload, arrhythmias, or the underlying myocardial disease, in which the latter seems to be the main factor contributing to RV dysfunction in patients with nonischemic dilated cardiomyopathy compared with ischemic cardiomyopathy, proposing the possibility of genetic predisposition in these patients (12).
Iglesias-Garriz et al. demonstrated that the presence of RV dysfunction in patients with HF with reduced EF (HFrEF) was associated with increased mortality and they also reported the prevalence of RV dysfunction in a meta-analysis of HFrEF been 48% (12, 13). Similarly, we found 47.3% of prevalence in HFrEF patients presenting with normal LV size. RV morphology is complex and its function depends on a complex interaction of RV free wall function, interventricular septum function, and interactions between the left and right hearts, that is the reason that makes RV function evaluation confusing by echocardiography (14). Based on current guidelines for the echocardiographic assessment of right heart (9), sonographers should measure multiple parameters, considering that there is no accurate single index to note RV performance for sure. TAPSE, RV S’, RVMPI, and FAC are feasible indices that we use in our routine echocardiography to assess RV systolic function. Nevertheless, the association of RV echocardiographic characteristics and RV function assessed by CMR were documented by some studies previously (15-17). In our study differently from TAPSE which did not show a manifest relationship with RVEF, all other three echocardiographic parameters including RV S’, RVMPI, and RVFAC favorably expressed RV function.
RVMPI is an index of combined RV systolic and diastolic function. Despite the load dependency of RVMPI, the high reproducibility makes it a proper index to estimate RV performance. Furthermore, the acceptable accuracy of RVMPI to assess RV performance was mentioned by other authors in different clinical situations (18-20). In parallel with other studies, Vizzardi et al. (21) documented that pulsed Doppler RVMPI > 0.38 is a predictor of cardiovascular death and hospitalization in HF patients with LVEF < 40% and NYHA class II.
RVFAC has been found to have a good correlation with CMR-RVEF in a variety of pathologies such as HF, myocardial infarction and pulmonary hypertension (22, 23). The main advantage of RVFAC is the declaration of not only longitudinal but also radial contraction of RV opposed to single motion in TAPSE and RV S’, however poor detection of the RV lateral wall in some patients is the Achilles heel of this method.
RV S’ is a measure of longitudinal RV function and could be obtained easily, albeit its angle dependency. Wang et al. (24) showed that RV S’ had the strongest correlation with RVEF measured by CMR from among other 2-D echocardiographic parameters, such a way that S’ < 8.79 cm/s is the best indicator of RVEF ≤ 20%.
In contrast, TAPSE failed to provide a good correlation with CMR-RVEF in our study. Similarly to RV S’, TAPSE also represents longitudinal function of RV and is load dependent. Several false positive and false negative results were mentioned for TAPSE in different conditions such as regional RV hypokinesia, pulmonary arterial hypertension (25), and post cardiac surgery (26). Damy et al. (27) indicated TAPSE measurement as an independent marker of poor prognosis in HF patients with reduced EF, in the same way as combined TAPSE and systolic pulmonary pressure which was defined by Guazzi et al. (28), whereas Carluccio et al. (29) showed that preserved TAPSE did not necessarily implicate good prognosis in HF patients as some of them had impaired RV function when assessed by RV longitudinal strain, associated with 2-fold increased risk of events.
The RV dysfunction score proposed by Kamimura et al. (7) in pulmonary arterial hypertension is a composition of four conventional feasible and reproducible echocardiographic indices which could be of great help for detection of impaired RV function in a variety of pathologies that may affect RV like heart failure patients with normal or dilated LV size. We found a strong correlation between RVEF obtained from CMR and this simple and applicable scoring system in HNDC patients, suggesting the RV scoring system to be used in the ordinary evaluation of RV performance in HF patients.
5.1. Conclusions
In conclusion, we found RV dysfunction in about half of HNDC patients in spite of their normal RV size, similarly to the DCM group that was reported in previous studies. RV dysfunction score using conventional echocardiographic parameters was a good predictor of RVEF assessed by CMR. Finally, it is hoped that this document lays out future researches particularly by applying RV 3-dimensional (3-D) echocardiographic parameters to evaluate 3-D RVEF as well.
