


1. Introduction
Embryologically, the development of renal veins comprises multiple steps, making it a complex process. First, two renal veins, namely ventral and dorsal, are generated by the fusion of the supra- and subcardinal veins. Over time, with the regression of the dorsal vein, only the ventral vein remains and forms the renal vein (1). Variations of renal veins result from anomalies of this process (2). Naturally, duplicated renal veins, which are usually asymptomatic and incidentally detected when imaging for other reasons or during operation or autopsy, are the most common variations of the renal vein (3).
Ordinarily, the drainage of the kidneys is through the left and right renal veins, both draining to the inferior vena cava (IVC). The course of the right renal vein is shorter and more straightforward; it opens directly into the IVC, but the left renal vein opens into IVC after passing the space between the abdominal aorta and the superior mesenteric artery (2). The absence of the right renal vein is very rare, and to date, only 3 cases have been reported (4-6). Another case of marked right renal vein hypoplasia has also been recently reported (7). Here, we report a case of the absent right renal vein with a unique pattern of drainage.
2. Case Presentation
A 25-year-old female patient with abdominal pain was referred to the radiology clinic for abdominopelvic computed tomography (CT) with oral and intravenous contrast. On CT images, the right renal vein was absent. The drainage of the right kidney was through the upper pole to the suprarenal vein and thereafter to the right gonadal vein (Figures 1 and 2) and IVC. Some suprarenal veins were drained to the gastroepiploic branch of the superior mesenteric vein via collaterals (Figure 3). The IVC diameter, especially the intrahepatic portion, decreased. An increased diameter of azygos and hemiazygos veins was observed due to blood drainage from the left renal vein and left common iliac vein through suprarenal and lumbar vessels (Figure 4).
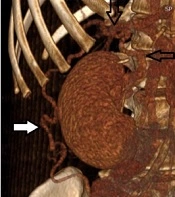
. Tortuous right suprarenal vein (down black arrow). Drainage of the suprarenal vein into the right gonadal vein (white arrow)")
Drainage of the right kidney through the upper pole into the suprarenal vein (left black arrow). Tortuous right suprarenal vein (down black arrow). Drainage of the suprarenal vein into the right gonadal vein (white arrow)
; right gonadal vein (right arrow). B, Right suprarenal vein joining the gonadal vein (right arrow); gonadal vein (left arrow)")
A, The course of the right suprarenal vein to drain into the gonadal vein (left arrow); right gonadal vein (right arrow). B, Right suprarenal vein joining the gonadal vein (right arrow); gonadal vein (left arrow)
; the gastroepiploic branch of the superior mesenteric vein (down arrow). B, Collateral vessels of the right suprarenal vein (left arrow); the lateral branch of the left renal vein, which passes through the aortic hiatus of the diaphragm and drains into the left hemiazygos vein (right arrow).")
A, Collateral vessels from the right suprarenal vein go down and run along the inferior margin of the right lobe of the liver and then turn up to the gastroepiploic branch of the superior mesenteric vein (up arrow); the gastroepiploic branch of the superior mesenteric vein (down arrow). B, Collateral vessels of the right suprarenal vein (left arrow); the lateral branch of the left renal vein, which passes through the aortic hiatus of the diaphragm and drains into the left hemiazygos vein (right arrow).
 and hemiazygos vein (B)")
Increased diameter of azygos vein (A) and hemiazygos vein (B)
3. Discussion
Although right renal vein variations are more common compared to the left renal vein (6), to date, only 3 cases of absent right renal veins with various patterns of drainage (4-6) and 1 case of significant right renal vein hypoplasia have been reported (7). The first case of congenital absence of the right renal vein was reported by Pinggera et al. in 2003 (6). Their patient was a 48-year-old woman who emergently presented with right flank pain. In this patient, the right renal vein originated from the renal hilum and drained into the right ovarian vein emerging from an ovarian venous plexus, which then flowed into IVC (6).
Another case of congenital absence of the right renal vein was reported by Bozlar et al. in 2008. The patient was a 25-year-old man who was radiologically evaluated for microscopic hematuria. In this patient, venous drainage of the right kidney was from the lower pole through an ascending collateral lumbar vein into IVC (4).
The third report was a case of the absent right main renal vein, with venous drainage of the right kidney from the hilum into an abnormal right adrenal gland venous plexus (5). Recently, a case of the hypoplastic right renal vein was reported by Fontana et al. (7). In this case, a dilated and tortuous vein originating from the hilum of the right kidney and draining to the right spermatic vein was responsible for right kidney drainage. However, a thin vein representing a remnant of the right main renal vein was also observed, which originated more cranially than the previous one from the hilum (7).
Our case is most comparable with a case reported by Kim et al. since, similarly, the drainage of the right kidney was to an aberrant right adrenal gland plexus in their case (5). However, in our patient, the drainage of the right kidney was through the upper pole, while in their case, it was through the hilum. Also, consistent with our findings, the drainage of the right kidney was to the right gonadal vein in almost all previous case reports (5-7); nevertheless, the origin and course were different.
3.1. Conclusions
The absence of the right renal vein is very rare, and to the best of our knowledge, drainage from the upper pole into the ipsilateral gonadal vein has not been previously reported in the literature.
