1. Background
Hepatitis E virus (HEV) is a single-stranded RNA virus with a size of nearly 27 - 34 nm that is classified as an Orthohepevirus genus (the Hepeviridae family) (1). It is a quasi-enveloped virus (by lipid membrane) in blood, and bile and feces are non-enveloped (2). The genome of the virus consists of a 5’-untranslated region (5’-UTR), three open reading frames (ORF1-3), and a 3’-UTR that terminated by a poly (A) tract (1). Genotypes 1 and 2 of hepatitis E are human viruses, which are highly endemic in several parts of Asia, Africa, the Middle East, and Mexico. There are nearly 3.4 million cases of acute hepatitis E resulting in 70,000 deaths due to acute liver failure annually (2-4). HEV transmits through contaminated water and food and can cause an asymptomatic simple infection or death. Its prevalence is higher in tropical and subtropical areas, particularly due to the higher consumption of raw seafood. Genotypes 3 and 4 of hepatitis E are zoonotic viruses and can infect humans and pigs (5, 6). It is also reported that hepatitis E can be transmitted to humans with a subclinical infection presentation through blood transfusion and organ transplants (7-9).
The prevalence of anti-HEV IgG is high in recipients of renal transplant (10), or patients with a severe immunodeficiency disorder, such as HIV or those who have chemotherapy. Chronic hepatitis E infection is rare and usually observes in patients with a suppressed immune system (7, 11). The geographical distributions of HEV genotypes are different. So that most of the infections caused by genotype 1 are in Asia and Africa. For genotype 2, the majority of infections are in Mexico, Nigeria, and Namibia, while infection with HEV genotypes 3 and 4 are reported in the USA, Argentina, European countries, Japan, and China (12). According to conducted studies, HEV infection is endemic in Iran, and its prevalence is higher among older ages and special groups with high-risk behaviors (5, 6, 13, 14). Thalassemia patients, who receive frequent blood transfusions, are at increased risk of transfusion-transmitted infections (15, 16). HEV can be transmitted through blood transfusion and can induce chronic infection in immunocompromised individuals. Besides, it can cause acute or chronic liver failure. So, in the current study, the presence of HEV infection in multi transfused patients was investigated.
2. Objectives
The current study aimed to estimate the prevalence of hepatitis E virus infection as an emerging virus among thalassemic patients in Tehran, Iran.
3. Methods
In this study, 110 serum samples of thalassemia patients from the Clinical Lab of the Tehran Blood Transfusion Organization that were taken during 2019 were selected. Screening tests of the selected thalassemia patients were negative (e.g., for HBsAg, HIV-Ab, and HCV-Ab). After receiving informed consent from participants, a questionnaire was given to them, which comprised of information regarding age, sex, marital status, occupation, and the history of blood transfusion, surgery, or hospitalization. The present study was approved by the Ethics Committee of Shahid Beheshti University, Tehran, Iran (no.: IR.TMI.1394.6).
3.1. Serological Assay (ELISA)
All serum samples were assessed for the presence of total anti-HEV antibodies (IgG and IgM) by using HEV Ab ELISA kit (Dia.pro, Diagnostic Bioprobes, Italy) according to the manufacturer’s instruction. To confirm the initial results, using the same kit, all positive samples were tested again.
3.2. Nucleic Acid Extraction
Viral RNA was extracted from serum samples using high pure viral Nucleic Acid Kit (Roche) based on instruction manuals, and the concentration of the extracted RNA was determined by spectrophotometer (WPA England).
3.3. cDNA Synthesis and RT-PCR
To synthesis the cDNA, the Easy cDNA Synthesis kit (parsTous Biotech) was used. First, 10 µL of 2× Taq premix was added to the micro-tube. Then, 1 µL from the each 10 µm primer (forward and reverse), 2 µL of the extracted viral RNA and 5 µL of water, nuclease-free were added to the microtube with a total volume of 20 µL. cDNA was synthesized for 10 minutes at 25°C, one hour at 50°C and heating at 70°C for 10 minutes. Subsequently, the nested RT-PCR amplification was performed with Emerald Max PCR master mix (Takara bio-kit, USA) containing 10 µL of 2× master mix,1 µL of 10 µm outer primer 1 and 1 µL of 10μm outer primer 2, 6 µL DDW and 2 µL of cDNA by thermocycler instruments (Corbett). The amplification was performed according to the following conditions: an initial cycle with five minutes of denaturation at 94°C, followed by 35 cycles of denaturation for 30 sec at 94°C, annealing for 30 sec at 55°C, and extension for one minute at 68°C, followed by 72°C for 5 minutes. For detection of the open reading frame 2 (ORF2) region of the HEV genome, the nested RT-PCR amplification was carried out in two rounds with two primer pairs. The primers (outer primer1, 5’-GAGGCAGGCACAACTAAAGC-3’and (outer primer2, 5’-AAGAAGGGGGGCACAAG-3’) were used in the first round of PCR. Then 2 µL of the first-round PCR product and 1 µL of inner primers were utilized in the second round of PCR. Secondary PCR primers were inner primer 3, 5’-GCA CCG GGT CGC TAT TTC-3’ and inner primer 4, 5’-TGA AGC TCA GCG ACA GTA GA-3’ (17). The amplification products of second-round were electrophoresed on a 1.5% agarose gel containing 0.5× TBE buffer, stained with 1.5 µL DNA green viewer, and photographed under UV light. Set-up PCR was performed using a positive control (a synthesized plasmid containing the full-length ORF 2 of the hepatitis E genome) (Takaposist Company).
3.4. Statistical Analysis
Analyses were performed using the SPSS software version 21. To assess the association between different factors, the chi-square test was used. The level of significance was set at 5%.
4. Results
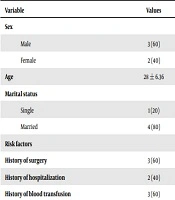
All serum samples were assayed for HEV total antibodies (i.e., IgG and IgM). The results of ELISA showed that 5 (4. 5%) out of 110 serum samples were positive for anti- HEV Ab. On analyzing results of ELISA IgG and IgM with regards to baseline data (gender, age, education, marital status, and job) and risk factors (Table 1), no statistically significant difference was observed (P = 0. 5). None of the samples was positive for HEV RT-PCR; therefore, the prevalence of HEV-RNA in thalassemic patients was determined at about 0.0%. There was no significant association between the prevalence of anti-HEV with the number of blood transfusions, sex, age, marital status, occupation, surgery, or hospitalization.
Table 1.
Frequency of Anti-HEV Ab Positive in Patients with Beta-Thalassemiaa
| Variable | Values |
|---|---|
| Sex | |
| Male | 3 (60) |
| Female | 2 (40) |
| Age | 28 ± 6.36 |
| Marital status | |
| Single | 1 (20) |
| Married | 4 (80) |
| Risk factors | |
| History of surgery | 3 (60) |
| History of hospitalization | 2 (40) |
| History of blood transfusion | 3 (60) |
aValues are expressed as No. (%) or mean ± SD.
5. Discussion
Hepatitis E virus, as an emerging infectious agent, causes transmission of HEV via the blood transfusion and development of chronic hepatitis E in patients who receive solid organ transplantation. The blood transmission of HEV is reported in Japan, England, France, and Saudi Arabia (18-22). However, the fecal-oral route is the main mode of transmission in Iran, but other routes of transmission, such as blood transfusion in individuals with multiple transfusions (e.g., thalassemia patients), are a concern. A meta-analysis study (14) reported that the overall seroprevalence of HEV is about 10% in Iran. In blood donors, the seroprevalence of hepatitis E ranges from 4.5% to 14.3% (23, 24). The risk of transmitting HEV infection via transfusion is due to the presence of HEV RNA in asymptomatic healthy blood donors. Tedder et al. (25) reported that the lowest viral dose required for HEV infection is about 2 × 104 IUs, and the presence of the virus in 55% of blood components is enough for transmission. When more than 13 individual donor components are transfused, the transfusion risk of infection substantially increases (25). According to the results of the current study, the prevalence of HEV-RNA in thalassemic patients was 0.0%. Therefore, due to the low prevalence of HEV in thalassemia patients, it can be concluded that blood transmission of HEV is not an important route, and other routes such as oral and fecal infections seem to be the main route of HEV transmission among thalassemia patients. Also, the findings show that blood transfusion is not a risk factor for HEV transmission among thalassemia patients in Iran. Although the risk of blood transmission of the virus is low, the importance of this infection should not be ignored among the transplant recipients, immunocompromised patients, and pregnant women. One of the limitations of this study was the low number of samples, so it is necessary to conduct a study with a larger sample size.
5.1. Conclusions
The results of the current study revealed that the frequency of HEV-RNA in thalassemic patients is zero. Therefore, the risk of blood transmission of HEV infection among thalassemia patients is low in Iran. However, the possibility of chronicity of HEV infection in solid organ transplant and immunocompromised patients receiving blood should be considered.
