


1. Background
The developmental approach to economic growth focuses on improving the quality of life and the capacity of human resources at all levels of production. Implementation of policies related to the health sector in developed and developing countries is of particular importance in ensuring and guaranteeing sustainable development and has challenged the important part of the government budget deficit due to high health expenditures (1). The mortality rate of children under five is of particular importance because it is often related to the community’s general health, the family’s living conditions, the health of the mother, and the economic status of the head of the household. Many thinkers in social science refer to the under-five mortality index as an indicator of social development from a socioeconomic perspective (2). In this regard, Shimouchi (3) and Nobles et al. (4) studied the influence of macroeconomic variables on health status and mortality rates and confirmed the relationship between under-five mortality and socioeconomic variables. According to the World Bank reports, about 3.74% of Iran’s gross domestic product in 1995 was spent on the health sector activities, reaching about 6.89% in 2014; therefore, the significant growth of this index shows the importance and the need for more attention to health by governments, including in Iran (5).
1.1. Human Development Index and Mortality Rate
Human development means attaining an acceptable level of health, knowledge, and ability to organize life and the primary purpose of development is to benefit people from improved quality of life and human development standards. Human development is the process of expanding human opportunities and capabilities (6). The human development index (HDI) is the geometric mean of the normalized indices for all three components of this index. The first criterion is the health or life expectancy index at birth, which encompasses the health aspect of life. The second criterion of the HDI includes the quality aspects of education, such as the literacy rate in society. The third criterion is the per-capita gross national income and income-generating employment (7). Alijanzadeh et al. (8) studied the factors influencing mortality rate in 135 countries in 2015 and showed a statistically significant negative relationship between the HDI status and the under-five mortality rate.
1.2. Per-capita Income and Mortality Rate
The reality of the economic life of developed and developing societies shows that with the growth of industrialization and urbanization, people’s real incomes in society increase, which increases the demand for public expenditure on social services, like education, health, and culture (9). The improvement of indicators such as GNI per capita pushes the community towards public health, adequate health care, and better nutrition. Nishiyama (10) examined the effects of GDP per capita on under-five mortality rates in 83 developing countries over 40 years using panel data and concluded that although economic growth broadly reduces mortality rate, its effects on child mortality are asymmetric and ambiguous during the boom and recession periods.
1.3. Education and Mortality Rate
The relationship between education and mortality is difficult to definitively establish due to the endogenous nature of the mechanistic pathways through which education contributes to improving health and reducing mortality (11). Acquiring education leads to better human, social and cultural capital in the population, which is associated with better health outcomes (12). In addition, education would positively impact levels of social engagement, an essential factor in creating more cohesive, safe, and healthy societies. It is also argued that a prosperous country has a high level of education, overall high HDI, and a high per capita income, which is the case for developed countries (13). Cutler et al. (14) emphasize the quality of education and its positive influence on health after examining the factors influencing community health.
1.4. Public Spending and Mortality Rate
Public spending is necessary but not sufficient. A sufficient condition for public expenditure is the effectiveness of government and the quality of bureaucracy that determine whether public expenditure has a significant impact on the quality of health outcomes in society (15). One of the biggest challenges for governments in the health sector is financing and budgeting. Health-related expenditures usually include insurance, medical, and pharmaceutical expenditures (16).
Issa and Quatara (17) studied 160 countries and highlighted the role of the government in reducing mortality rates, suggesting that the government’s efforts towards efficiency increase the health quality of mothers, leading to under-five children’s health. Moreover, David (18) examined the relationship between infant mortality and public health expenditure in Nigeria from 1980 to 2016 using the ARDL method and concluded that private and public health expenditure, immunization, and external health resources significantly negatively affect child mortality in the long and short run.
1.5. Urbanization and Mortality Rate
Usually, the city’s capacity is limited in many ways to meet citizens’ expectations of well-being, and the health care centers cannot increase the urbanization rate as quickly. High rates of urbanization, especially in developing countries, can lead to poor health care and increased mortality; increasing population density in urban areas leads people to have less access to health and education services (19). Barrett (20) studied the causes of infant mortality in Nigeria and showed that under-five mortality increased from 1979 to 1983 and from 1999 to 2003, primarily due to high mortality rates and more stressful life in urban areas.
1.6. Income Inequality and Mortality Rate
In general, when income and wealth are distributed more equitably, and inequality is reduced, more people can afford the costs of health care, proper nutrition, and private hospitals, leading to increased health and well-being. Unequal distribution of income and wealth measured by the Gini inequality index significantly impacts health status and health spending. Income inequality exacerbates health expenditures, especially in lower-income groups (21).
The main objective of the present study was to investigate the relationship between macro-socioeconomic variables and mortality rate in MENA countries and find a clear answer to the question of whether the HDI and income inequality are the main factors affecting mortality rate in MENA countries. In addition, the possible and meaningful influences of other essential variables such as urbanization rate, government health expenditure, and per-capita gross national product were also investigated.
2. Methods
The present study used the panel data analysis method to investigate the impact of macroeconomic variables such as HDI, Gross Domestic per capita (GNI) based on purchasing power (2011 PPP $), urbanization rate, government health expenditure as a percentage of GDP, and income distribution inequality index (Gini) on the under-five mortality rate. The panel data analysis used in this study is a subset of longitudinal data in which similar information was collected for each MENA country and entered into the research model presented in Equation 1.
MRit = β0 + β1 HDIit + β2GNIit + β3HEPit + β4INEit + β5 URit +εit
where MR indicates the under-five mortality rate, HDI is the human development index, GNI indicates gross national income, HEP indicates government health expenditure as a percentage of GDP, INE indicates income distribution inequality, and UR is the urbanization rate in each country (i) in a specific year (t). The relevant data are collected from the MENA countries’ data recorded in the World Development Indicator (WDI) for 2003 - 2019. The select MENA countries in the study are Bahrain, Egypt, Iran, Jordan, Kuwait, Lebanon, Oman, Qatar, Saudi Arabia, and the UAE.
3. Results
The normality test results are reported in Table 1, which shows the normal distribution of research variables (P-value > 0.05).
| Values | |
|---|---|
| Jarque-Bera | 3.78 |
| Mean ± SD | 9.36 ± 26.53 |
| P-value | 0.15 |
Before estimating the research model, the Limer-F test was performed to determine the type of panel data estimation or select either panel data or pooling data for model estimation. The results of the Limer-F test are summarized in Table 2, showing that the model is fit for panel data analysis.
| Effects Test | Statistic | df | P-Value |
|---|---|---|---|
| Cross-section F | 53.072 | (9,150) | 0.000 |
| Cross-section chi-square | 239.035 | 9 | 0.000 |
Further, the Hausman test was then used to determine fixed-effects or random-effects methods were sufficient to estimate the research model. The results of the Hausman test are summarized in Table 3, showing that the fixed-effects method is suitable for model implementation.
| Test Summary | Chi-square Statistic | Chi-square df | P-Value |
|---|---|---|---|
| Cross-section random | 4.800 | 5 | 0.028 |
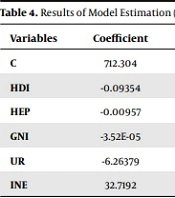
Finally, according to the Hausman and Limer-F test results, the panel data with a fixed-effects model was used to estimate the effect of independent variables in this study. By adopting the EGLS test, the presence of heteroscedasticity was ruled out, as shown in Table 4.
| Variables | Coefficient | Std. Error | t-Statistic | P-Value |
|---|---|---|---|---|
| C | 712.304 | 50.7312 | 14.0407 | 0.0000 |
| HDI | -0.09354 | 0.01285 | -7.27785 | 0.0000 |
| HEP | -0.00957 | 0.15978 | -3.97805 | 0.0095 |
| GNI | -3.52E-05 | 0.12153 | -2.28934 | 0.0027 |
| UR | -6.26379 | 0.44931 | -13.9406 | 0.0000 |
| INE | 32.7192 | 2.80800 | 6.43455 | 0.0034 |
a R-squared = 0.966203; P-value = 0.0034.
Based on the t-statistic and the standard error of all variables, the null hypothesis was rejected, and thus, all variables had a significant effect on the under-five mortality rate when tested at the 5% error level. Moreover, since the P-value of all variables is less than 0.01, there is strong evidence against the null hypothesis. On the other hand, the result showed that the R-squared is 0.96 (P-value = 0.0034). It is a statistical measure representing the proportion of variance for a dependent variable explained by independent variables in a regression model. Thus, the R-squared statistic presents that approximately 96% of the observed variation is due to the model’s inputs. The factors affecting the under-five mortality rate showed that an increase in GNI per capita, health expenditure share, urbanization rate, and improvement in human development index could reduce the under-five mortality rate in the select MENA countries. In contrast, income distribution or inequality index worsens health status and increases mortality.
4. Discussion
Most countries in the MENA region have many similarities in their economic situations, so the issues raised and analyzed can significantly benefit them. The study findings related to the HDI index also emphasize improving the quality of education and how people use the facilities available in the community. Increasing personal knowledge and skills will help people use their resources better and avoid risks. Increasing the knowledge level of people in the community, especially mothers, and using more technical knowledge in the provision and use of health services can significantly reduce mortality rates. In addition, education generates more income and higher wealth in the future, and increasing the education and awareness of family members, especially mothers, reduces the risk of child death because educated mothers learn more about how to care for their children.
It is also important to pay attention to the growth rate of urbanization because an appropriate growth rate of urbanization, following the natural transfer of surplus labor from rural to urban areas or transitional process from agricultural products to industrial high-tech products would have a positive impact on reducing the under-five mortality rate. Otherwise, high urbanization rates and expansion of densely populated cities without expansion of education, health, and care facilities may have direct and indirect adverse effects on mortality. With the development of facilities and access of community members in urban areas, along with the admission of migrant workers from rural areas to urban areas, a decline in the under-five mortality rate can be expected.
Usually, governments are familiar with the three tasks of optimal allocation of resources, equitable distribution of income, and economic stability and consider these duties for the people’s good. The findings of this study indicate that the unequal distribution of income and wealth in society creates a deep gap between classes and makes the poor even poorer. Poverty and inequality in income distribution increase the mortality rate. Therefore, one of the necessary measures for the government is to adopt a fiscal policy to distribute more revenue through expenditure.
4.1. Conclusions
The promotion of the HDI, which is an international standard index, emphasizes that with economic growth and increased per capita income, poverty can be reduced, and access to health care and maternal and under-five health can improve. Increased per capita income provides better health by improving living conditions, such as access to clean drinking water, decent roads, and adequate nutrition, because increased per capita income creates more purchasing power, which can improve the quality and quantity of health care. This study showed that the HDI significantly improves the income-education-health structure, and strengthening this structure can always lead to mortality reduction, especially among children under five.
The study highlights the critical role of per capita GDP growth and higher per capita income of people in better access to health facilities. As the rate of economic growth increases, GDP increases, so does the share of people in national economic output. Increasing the per capita income of people increases the purchasing power of goods and services, including the demand for health services and care. This study confirms Wagner’s income-consumption theorem, which states that as society grows and develops, national income increases, and thus people’s consumption expectations for goods and welfare services increase. At this stage, the role of government in providing welfare facilities to the people, including their health and care needs, usually increases with government expenditure and through appropriate taxation policies; the government meets society’s expectations by providing welfare services.
Improving the income inequality index plays a vital role in the effectiveness of government fiscal policy. For this reason, policymakers in MENA countries need to think about how to improve people’s income and living conditions to escape from poverty. Therefore, it is recommended that by enhancing social capital and increasing the motivation of citizens, planners first collect appropriate sources of income, including taxes, and then invest the income in productive infrastructure to increase GDP and growth rate, plan to create valuable jobs to increase per capita income, reduce poverty, and finally achieve equitable distribution of wealth. Obviously, by increasing the rate of economic growth, employment, and per capita income, people in the community will have access to health services, which ultimately leads to a reduction in the under-five mortality rate. This study on developing MENA countries puts a strong emphasis on the role of good governance in expanding educational, health, and business facilities of society as a requirement for the growth and development of the community, promotion of the human development index, and finally, the reduction of the mortality rate of children under five years old.
