1. Background
Coronary artery disease (CAD) is the first leading cause of death and the third most prevalent disease in most developed and developing countries (1-3). Mortality rate has been reported as 331 per 100000 individuals/year in males and 203 in females, and this mortality rate included 35% of total mortality rate in Iran (4, 5). One person every 39 seconds or 2300 individuals per day die due to cardiovascular disease (6, 7). Moreover, in 2006, about 25 million people lived with coronary heart disease and stroke in the USA (8). However, CAD is increasing around the world due to the phenomenon of modernization, technological progress, and growing underlying risk factors (9). Hypertension and diabetes are on the rise, and have been linked with CAD occurrence. Patients with diabetes are 2 to 8 times more likely to develop cardiac events in comparison with other patients (9, 10). In addition to economic costs, CAD can lead to social and health problems (11). Therefore, many countries have adopted the policy of primary and secondary prevention and screening to identify patients at moderate and high risk (3, 12, 13). In addition to establishing the diagnosis, cardiovascular imaging plays an important role in screening and estimation of risk of CAD (14).
Cardiac catheterization and angiography is the gold standard method for diagnosis of CAD (15, 16). Angiography is used in determining the extent and severity of cardiac involvement and medical treatment policy, surgery, and invasive interventions in symptomatic patients (17). Also, practitioners use angiography to diagnose and treat patients with high risk CAD (9). However, coronary angiography is a costly procedure and Myocardial Perfusion Imaging (MPI) has been the preferred method in secondary prevention of CAD (17). Myocardial Perfusion Imaging can be applied as an alternative and appropriate diagnostic method to other non-invasive procedures (18). Also, MPI is the recommended method for determining the severity of myocardial ischemia and prognostic value for cardiovascular events and can affect the therapeutic optimal approach (19, 20). However, there is a possibility of obtaining false positive results with myocardial perfusion imaging in individuals with normal angiography (21-23). In the study of Schuijf et al., myocardial perfusion imaging compared to invasive coronary angiography had less accuracy for detecting CAD (24), while in another study by Li et al., there was no significant difference between sensitivity, specificity, and accuracy of MPI compared to Computerized Tomography (CT) coronary angiography in diagnosing CAD, and both had good diagnostic performance for CAD (25). Tamarappoo et al. showed that extent and severity of myocardial perfusion defects, measured by CT coronary angiography had a strong similarity with SPECT myocardial perfusion imaging (26).
Since the effect of CAD risk factors, including diabetes and hypertension on perfusion imaging results after compliance with angiographic findings, and also the relationship with angiographic results in terms of scoring and the affected area have not been investigated so far and most studies compared myocardial perfusion imaging with CT angiography as a noninvasive method, thus, this study aimed at comparing MPI with catheter angiography for examining coronary arteries.
2. Methods
In this study, patients with stable angina pectoris, who were referred to Kowsar hospital, Semnan (Iran) from May 2013 to April 2014, were recruited. The patients with age range of 30 to 80 years and positive MPI, confirmed by a cardiologist, were selected using convenience sampling. Also, patients with unstable angina, chronic heart failure, myocardial infarction, revascularization, aortic insufficiency, aortic stenosis, cardiomyopathy, and hypertrophic and hypertension pulmonary disease were excluded. Ethical approval was obtained for this study from the ethics committee of the Semnan University of Medical Sciences. All recruited patients provided informed written consents.
2.1. Myocardial Perfusion Imaging
All patients were examined at the nuclear medicine center of Kowsar hospital by Gated Spect myocardial perfusion imaging method on two consecutive days, applying pharmacological stress and exercise, using Siemens camera (large field LEAP) and TC99m-MIBI radiopharmaceutical apparatuses. All of the heart scans were done using the E Cam machine, manufactured by Siemens, Germany. Scans were conducted by the internal medicine assistant, in cooperation with the nuclear medicine expert from the nuclear medicine department.
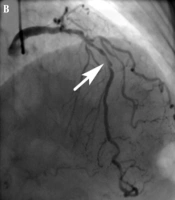
2.2. Coronary Angiography
After perfusion scan, angiography was performed within 3 months. All angiographies were recorded at Kowsar hospital of Semnan city, using Germany Siemens Axiom Artis angiography apparatus with cooperation of the cardiologist.
2.3. Data Collection
Demographic and therapeutic data were collected using a questionnaire. Nuclear medicine scans were classified by the nuclear medicine specialist as involvement of the inferior, anterior, lateral and septal walls, and results were categorized as mild, moderate, and severe. Angiographic results were documented by the cardiologist and the types of coronary artery involvement included left coronary circumflex (LCX), right coronary artery (RCA), and left artery descending (LAD), and significant stenosis was considered as narrowing of the vessel lumen by more than 50% (7).
2.4. Data Analysis
The SPSS 16.0 software was used for data analysis. Descriptive statistics were used to describe data and to analyze the data; Chi-square test and Spearman and Pearson correlation coefficient were used. The sensitivity, specificity, positive, and negative predictive values were also calculated. The significance level was 5%.
3. Results
In this study, 155 patients with stable angina were enrolled in the study. The mean age of the patients was 58.3 ± 11.5 years. Minimum and maximum age was 33 and 80 years, respectively, and 82 (52.9%) individuals were male while 73 (47.1%) were female. The MPI results showed that the lateral wall (44.5%) was the most common affected wall. Also, 69% of patients had the complication in 1 wall, 25.2% in 2 walls, 5.2% in 3, and 0.6% in four walls of the heart (Table 1).
Table 1. Distribution of Affected Areas in Perfusion Imaging
| Considered Site | Count | Percentage |
|---|---|---|
| Inferior | 37 | 23.9 |
| Anterior | 20 | 12.9 |
| Lateral | 69 | 44.5 |
| Septal | 34 | 21.9 |
| Apex | 53 | 34.2 |
| Total patients | 155 |
Angiographic results in 47.7% (n = 74) of patients were abnormal. In 35 patients (47.3%), 1 vessel, in 27 patients (36.5%) 2 vessels, and in 12 patients (16.3%) 3 vessels were affected. The most common affected vessel was related to LAD (42.6%). Among the patients, 46 males (56.1%) and 28 females (38.4%) had at least 1 of the vessels affected on angiography and this difference between the genders was statistically significant (P = 0.027). There was a significant correlation between the involvement of at least 1 vessel and age (r = 0.458 and P = 0.001). Scan results on all the walls had low sensitivity (less than 50%). There was a specificity of 80%, positive predictive value of 64%, and negative predictive value of 65%. In patients, who had anterior wall perfusion defect in their scans, 70% had an affected vessel in angiography. However, considering those who did not have a defect in their anterior wall perfusion, in 44.4% coronary involvement was observed by angiography, the difference of which was statistically significant (r = 0.413 and P = 0.028). In patients, who had septal wall perfusion defect, according to the MPI finding, 64.7% of them and also, in those who did not have septal wall perfusion defect, 43% had coronary involvement in angiography, the difference of which was statistically significant (r = 0.541 and P = 0.025) (Table 2).
Table 2. Sensitivity, Specificity, and Positive and Negative Predictive Value of Perfusion Imaging
| Scanned Site | Perfusion Scan Result | Angiography Resulta | P Value | Sensitivityb | Specificityb | Positive Predictive Valueb | Negative Predictive Valueb | |
|---|---|---|---|---|---|---|---|---|
| Positive | Negative | |||||||
| Inferior | Positive | 17 (23) | 20 (24.7) | 0.802 | 23.0 | 75.3 | 45.9 | 51.7 |
| Negative | 57 (77) | 61 (75.3) | ||||||
| Anterior | Positive | 14 (18.9) | 6 (7.4) | 0.028 | 18.9 | 92.6 | 70.0 | 55.6 |
| Negative | 60 (81.1) | 75 (92.6) | ||||||
| Lateral | Positive | 33 (44.6) | 36 (44.4) | 0.985 | 44.6 | 56.6 | 47.8 | 52.3 |
| Negative | 41 (55.4) | 45 (56.6) | ||||||
| Septal | Positive | 22 (29.7) | 12 (14.8) | 0.025 | 29.7 | 85.2 | 64.7 | 57.0 |
| Negative | 52 (70.3) | 69 (85.2) | ||||||
| Apex | Positive | 31 (41.9) | 22 (27.2) | 0.053 | 41.9 | 72.8 | 58.5 | 57.8 |
| Negative | 43 (58.1) | 59 (72.8) | ||||||
| At least 2 of the above locations | Positive | 34 (45.9) | 14 (17.3) | - | 45.9 | 82.7 | 70.8 | 62.6 |
| Negative | 40 (54.1) | 67 (82.7) | ||||||
| At least 3 or more | Positive | 8 (10.8) | 1 (1.2) | - | 10.8 | 98.8 | 88.9 | 54.8 |
| Negative | 66 (89.2) | 80 (98.8) | ||||||
aInvolvement of at Least One Coronary Artery; Values are expressed as No. (%).
bValues are expressed as number percent.
Also, 38.6% of the patients with mild scan score, 87.5% of the patients with moderate scan score, and 91.7% of the patients with severe scan score had at least one affected coronary on angiography. The correlation between scan score and angiography finding was significant (r = 0.501 and P = 0.001). The Pearson correlation test showed that the correlation between the number of involved vessels in the angiography and scan score was significant (r = 0.472 and P < 0.001).
4. Discussion
This study aimed at comparing the diagnostic value of MPI and coronary angiography, the results of which showed that the sensitivity of perfusion was less than 50%, positive predictive value was 64%, specificity 80%, and negative predictive value 65%.
In a study by Wang et al. (1995), MPI with SPECT, using the radiopharmaceutical agent Tc-99m sestamibi (MIBI), was analyzed. The sensitivity and specificity of this method for the diagnosis of CAD with the degree of stenosis being 70% < (in angiography) was 95% and 75%, respectively (27). Also, the sensitivity and specificity (accuracy) of MIBI scan in patients, who had angina, and in healthy controls was the same in the diagnosis of CAD. This study showed that Tc-99m MIBI myocardial perfusion imaging for the diagnosis of CAD in elderly patients could be an alternative to coronary angiography (27).
In the study of Hannoush et al. (2003), Positive Predictive Value (PPV) for myocardial perfusion scan was 91% and negative predictive value (NPV) was 86%. Also, in this study, myocardial scintigraphy later influenced the decision to perform coronary angiography (28). Elhendy et al. (2000) showed that the sensitivity of the scan to detect significant CAD was 95% with a specificity of 55% and accuracy of 88%, and also when the defect was considered reversible, specificity was 73% (29). Johnson et al. (2001) also found 88% sensitivity and 93% specificity, when they compared myocardial perfusion scans with angiography as the gold standard method (30). In another study by Vakili et al. (1995) conducted on 59 patients, SPECT MPI and angiography were performed for all patients, and sensitivity of 90% and specificity of 80% was obtained for myocardial perfusion imaging in comparison with angiography in the diagnosis of myocardial ischemia, respectively (31). Fard-Esfehani et al. (2007) also revealed that SPECT MPI had 91.2% sensitivity and 86.6% specificity in comparison with angiography and they concluded that based on the findings of this study, the sensitivity and specificity of myocardial perfusion imaging in nuclear medicine department was acceptable and could be very efficient in the diagnosis of patients (32). Shelley et al. (2012) in India applied myocardial perfusion SPECT imaging and angiography on 99 patients and eventually 87% sensitivity and 80% specificity for MPI was obtained. In this study it was concluded that abnormal perfusion revealed the hemodynamic significance of anatomic lesions on angiography and was able to show coronary atherosclerosis before clinical symptoms indication and played a major role in the decision to angiography; also a normal perfusion scan, which has rejected a normal ischemia, cannot rule out ischemic coronary artery disease (33). Fiechter et al. (2011) obtained a sensitivity of 87% and specificity of 67% for myocardial perfusion imaging (34). In all these studies, the sensitivity and specificity of myocardial scintigraphy was estimated at a high level, representing the diagnostic value of this method. In the present study, scanning sensitivity was obtained as 30% and specificity as 80%, although the specificity was similar with other studies, yet its sensitivity was much lower than other studies. Positive and negative predictive value of perfusion scan results was the same at 65% and 64%, respectively.
One limitation of the current study was the lack of investigation of the accessory coronary branches such as diagonal and underlying conditions such as diabetes and hypertension to compare the findings with other patients. Therefore, further studies are required in this regard. The strengths of our study were selecting the patients with positive perfusion scan by SPECT MPI and the same cardiologist, who performed the SPECT MPI and invasive coronary.
4.1. Conclusions
This study showed that MPI had a low sensitivity and high specificity. Further studies are recommended to determine therapeutic advantages of MPI.