



1. Background
Pragmatics is the use of language in interpersonal situations (1, 2), which includes people’s informal and formal encounters with friends and family as well as those in schools and workplaces. Pragmatics is a prominent research area in children with intellectual disability (ID) (i.e., those who have below-average intelligence and lack the skills necessary for a day-to-day living) (3-5). Development and use of pragmatic skills in everyday life is central to many questions concerning the quality of life of people with ID (6). These people need to have proper pragmatic skills to be able to have positive social interaction when they make friends, want to have intimate relationships, find a job, and participate in leisure activities (7-10). In addition, the development of pragmatic skills is related to the other areas of language (e.g., semantics and syntax) as well as social and cognitive development (11-13).
Language development and hence the pragmatic area have a close relationship to the social interaction as a dynamic factor (14, 15), since social interaction gives children opportunities to learn from their environment, practice the new language forms, and improve their linguistic and communicative skills (16). Sensitive responsiveness, joint attention, co-regulation, and an emotional component are the four important factors in interactions between persons with profound ID and their communication partners (17). However, not every person considers all these four factors during interaction, as people have different styles for responsiveness and assertiveness.
There is a functionalist perspective to study language development. The earliest proponents of this perspective argue that language originates out of the child’s need to progressively share more complex needs, requests, and feelings with people who are in their social environment. Some of them even believe in a reciprocal influences or transactional model of language development, which means that the caregivers affect and are affected by child’s behavior during the course of development (6). At first, the caregivers illustrate and imply the basic mechanism of conversation. When the child acquires these basics, this is the child’s utterances that shape the caregiver conversation. As children become more sophisticated in the basic rules of conversations and learn to rely on words instead of gestures during their interactions, the caregiver-child conversation starts to change gradually (6).
Fey introduced a protocol to assess socio-conversational skills in children and to consider these skills in intervention. According to his model, different speech acts such as requests, responses, asserts, and performative are calculated in a language sample taken from a dynamic interaction between child and a communication partner. Based on the child’s responsiveness and assertiveness, children can be categorized as: Passive conversationalist, active conversationalist, verbal non-communicators, and inactive communicator (Figure 1) (18). The responsiveness and assertiveness of communication partner can be evaluated by Fey’s model. However, if the communication partner is one of the parents, the term to categorize parents would be different.
")
Figure 1.
A scheme for profiling children based on their levels of social-conversational participation (18)
Four parenting styles could be defined based on parents’ responsiveness and demandingness: (1) authoritative style with high levels of both responsiveness and demandingness; (2) authoritarian style with low levels of responsiveness but high levels of demandingness; (3) permissive style with high levels of responsiveness but low levels of demandingness; and (4) uninvolved style with low levels of both responsiveness and demandingness (19, 20).
Learning the basic conversational rules needs an optimal level of cognitive abilities (21). Thus, the presence of ID may compromise the learning of conversational skills. There are studies with functional perspective that have investigated the development of conversation skills in children with ID, indicating that children with ID (mainly with Down syndrome) acquire the basic aspects of conversation (22, 23). They have confirmed that children with ID are successful in responding for clarification, producing utterances designed to prompt responses from a communication partner (e.g., statements, commands, comments, interrogations, answers, suggestions, and request), and considering the status of conversation partners during interactions. However, some aspects of their conversation environment restrict them to extend and use all conversational skills (6). However, these findings have been questioned by recent studies (24, 25).
Scudder and Tremain, and Brinton and Fujiki reported that children with ID were not as responsive as their typical peers were, and their requests were not as frequent as their typical peers (24, 25). Such discrepancies may be a result of the characteristics of participants (i.e., some included milder degrees of ID while some included more severe ones), the methodology they applied (i.e., some administered a task while some just analyzed a child-mother interaction), and the last possibility could be assigned to the definitions of their variables (i.e., considering only some of the specific repair behaviors vs. all of the responsiveness acts and requests). Therefore, it is ideal to implement a model that can combine assertiveness and responsiveness and facilitate judging both at the same time in a group of children with ID who are in similar non-verbal mental age.
Hatton (6) and Marfo (26), in review and commentary articles, provided details about the caregiver’s speech to the children with ID. They showed that these caregivers were more directive in caregiver-child communications than the caregivers of children without ID by particularly, controlling the mental age, chronological age, and language skills (22, 27, 28). Caregivers of children with ID usually adopt more dominant position (22) and play a controlling role during the child’s play (27). These studies indicated that these children were less contingently responsive to their caregiver teaching, and spent less amount of time to interact with their caregivers (22, 27). The same studies confirmed the existence of a negative relationship between caregivers’ non-facilitative directives (i.e., initiating a new topic without considering the child’s interest) and child language or cognitive abilities (26, 27, 29, 30). Recent studies have confirmed previous findings as the parents of children with ID are more controlling than the parents of children with typical development during interactions. However, recent studies have also found that caregivers’ speech is supportive for language development and caregivers integrate the contextualized and decontextualized speech into their mother-child interactions (31-34).
Most of these studies have recruited the families having children with Down syndrome, and, therefore, our knowledge is not enough about children with ID with other etiologies or unknown etiologies (i.e., etiologies other than genetics include 50% of children with ID (35)). The research focus, as well as the adopted methodologies have been different in related studies conducted in Iran (36-38). Ashtari et al. offered further details on all previous studies investigating the parenting style in Iranian culture, and confirmed that the mothers’ responsiveness positively affected the children’s language skills (38). A most recent study by Khanipour et al. indicated that parenting style (i.e., authoritative and permissive styles) had the potential to positively predict the semantic and syntactic development in typical Persian-speaking children (36).
To the best of our knowledge, no study had ever focused on the conversational skills of children with ID in Iranian culture. Moreover, it was difficult to generalize the findings about the conversational skills practiced in English-speaking world – which is a culture-based issue – to Persian-speaking children. Therefore, it was felt necessary to explore the conversational skills in Persian-speaking children with ID, find any similarity or difference among different cultures, as well as recognize, possibly, any particular intrusive style and develop effective intervention programs.
2. Objectives
Considering the value of conversational skills as a well-known area in pragmatics with positive effects on developmental aspects of children with and without ID, the present study aimed to:
- Identify the main role that children with ID play in conversation with a familiar person (here their mothers) adopting the Fey’s model;
- Define the major type of parenting style of children’s mothers during their interaction based on their responsiveness and assertiveness during the interaction;
- Find the correlation between conversational skills and common language indices.
3. Methods
3.1. Participants
A team, including a psychologist, two linguists, and four speech and language pathologists (SLP) participated in this study. Children with ID were selected through purposeful sampling from special needs schools in cities form Semnan province, including Mahdishahr, Semnan, and Garmsar cities with the exception of Shahrood city. Out of 34 children with ID who were initially selected for investigation, only 21 were eligible to be included in the present study. The eligibility of each child was checked by an experienced SLP using the provided documents. The inclusion criteria were children: With mental age between 4 and 5 years, diagnosed as ID by a pediatric psychiatrist, with no record of active neurological disorder such as epilepsy or seizure, specific sensory deficits such blindness or hearing loss, and determined to be monolingual (Persian users). Those children who were not able to talk or communicate were excluded from the study.
3.2. Procedure
In this cross-sectional study, children and mothers were evaluated using a comprehensive set of tests, including interviews to collect demographic information, a standardized language test, a conversational skills rating scale, and a test to examine the interaction between child and their mother. All steps of this procedure were administered individually. The language samples were collected during a 20-minute interaction that each child had with his/her mother in a free play context. Similar dolls, dollhouses, farm animals, and cars in different shapes and colors, available on the floor, were provided during the interaction. The children started playing and were free to choose any toys during the interaction. The SLP did not tidy up the room during interaction, but took notes and recorded all non-verbal answers and questions/requests.
All sessions were recorded, transcribed, and segmented according to the principles in the Fey’s socio-conversational analysis (39). In this model, the numbers of responses (i.e., response to attention, clarification, information, and action) was calculated in order to measure the responsiveness. All statements, comments, disagreements, as well as all types of requests (e.g., request to attention, clarification, information, and action) were combined to measure the assertiveness.
The middle ten minutes of the sessions were analyzed based on the time-based language sample cutting method. Half of the language samples were transcribed, segmented, and analyzed by a blind SLP to evaluate the reliability among raters. The agreement between raters were above 98%.
3.3. Tools
3.3.1. Leiter test
The psychologist evaluated each child’s cognitive skills using the Persian version of Leiter in 20 - 45 minutes. The test-retest reliability coefficient of the total score was above 0.70, and its Cronbach’ s alpha coefficient was above 0.70 (40).
Language Profile Monitoring Pack: Section 1 of the Assessment Profile of language skills in children aged 2;06-5;00 relating to the child’s and family background information (i.e., from family history to child’s development) was administered (41).
3.3.2. TOLD-P:3
The SLP administered the Persian version of the Test of Language Development (TOLD-P:3). The TOLD-P:3, with six core subtests and three supplemental subtests, evaluates different aspects of oral language. According to the manual, the SLP can combine the results of these subtests and obtain composite scores for the major dimensions of language: "Semantics and grammar; listening, organizing, and speaking; and overall language ability”. The composite score at or below 69 was considered as ‘very weak’ (42). Hasanzadeh and Minaei calculated the internal consistency coefficients of the subtests and reached to scores between 0.44 and 0.79. The criterion related validity was 0.40 - 0.70; the construct validity was 0.3 - 0.6; the factor analysis was found to be 0.64 - 0.79; and the discriminant power of the core subtests was above 0.9 (42).
3.3.3. Conversational Skills Rating Scale
The Persian version of conversational skills rating scale (Cronbach’s alpha = 0.9; CVR = 1, & CVI = 0.9) was applied to evaluate the mothers’ evaluation of their children’s pragmatic skills (43). Two different scores as "responsiveness score" out of ten items and "assertiveness score" out of 15 items, can be calculated. Average scores in each of the two scales of 4.8 or greater are considered as “well-developed” pragmatics; scores between 2.5 and 4.8 are regarded as “pragmatic skills are emerging” pragmatic competence; and those children with scores less than 2.5 are considered as “no or infrequent pragmatic skills” (43).
3.3.4. Vineland Social Growth Scale
To evaluate children’s ability to meet their practical needs and take responsibilities, the Persian version of the Vineland Social Growth Scale was administered. The SLP interviewed mothers to complete the form. This scale includes 117 items and has eight categories. The scale is based on what children are able to do in daily life. Scale items can be divided into eight categories (i.e., General, self-help, Self-help in eating, Self-help in dressing, Self-command, Employment, Linguistic communication, as well as Movement and socialize). Two scores are extracted as Social Age and Social Quotient (SQ). Social Quotient is the ratio between social age and chronological age. To be more precise, SQ as an index of social maturity could be calculated as social age divided by chronological age, and then the ratio is multiplied by 100 (social age/chronological age) * 100. A SQ is a concept parallel to an intelligence quotient, wherein a score of 100 indicates average performance for age, and scores less than 100 indicates below average functioning (44). The validity and reliability of this scale for Iranian population have been reported as satisfactory, and the Cronbach alpha has been above 0.9 (45).
3.3.5. Socio-conversational Analysis
In the first step, the turn was defined to facilitate segmenting the verbal acts. A turn was regarded as a time during which a single participant spoke within a typical and orderly arrangement in which participants spoke with minimal overlap and gap between them. The waiting time was considered two seconds; if any of the parties failed to use their turn that turn was marked as “no response”. The nonverbal responses were recorded as a proper responsive act.
The provided segments were labeled as a specific assertiveness or responsiveness behavior based on Fey’s model. The turns for each participant were counted, numbered, accumulated, and considered as “total turn” in each interaction. Then, the number of child’s turn was divided by the total turn and multiplied by 100 to calculate the percentage of child’s turns; similar approach was implemented to calculate the percentage of mother’s turns. Child’s assertiveness and responsiveness were calculated by dividing the number of each conversation acts over the child’s turns multiplied by 100. For child 1, for example, seventy turns were recognized. Out of these turns, mother possessed 36 turns (51.43%) and the child had 34 turns (48.57%). In this interaction, the number of requests was 36 (35 for the mothers and one for the child), and the number of responses was 34 (one for the mother and 33 for the child). This child's communicative behaviors were 2.94% as assertiveness and 97.02% as responsiveness. While both parties had almost similar number of turns, the child acted as a passive conversationalist.
To search the relationship between the conversational behaviors and some common language indices, mean length of utterances or MLU (calculated through dividing by the number of morphemes to the number of intelligible, complete, and grammatical utterances) (46), type-token ratio or TTR (calculated by dividing the number of different words to the total number of words) (46), number of different words (46), and simple sentence (consists of only one independent clause) and complex/compound sentence (includes two or more clauses either dependent or independent) were calculated.
3.4. Ethical Consideration
This study was completed according to the database of research and approved under ethics code: IR.SEMUMS.REC.1400.234. The informed consent was obtained by SLPs, and all families were assured of their anonymity and confidentiality of their information in all stages of the study. The families were also reassured that there would be no harm to or negative consequences for them or their children throughout the study, and they were allowed to withdraw from the study at any stage. The whole process of the clients’ participation was completed in a time and location convenient for the participants.
3.5. Statistical Analysis
The obtained data were analyzed using the statistical software IBM SPSS 24.0 for Windows (SPSS Corp, Chicago, IL). Mean, and standard deviation (SD) were calculated as the descriptive indicators for the outcome measures. The Shapiro-Wilk test was adopted to check the normal distribution assumption. The Spearman-rho was also employed to search for possible correlation between conversational skills and general language indices. A P-value of less than 0.05 was considered significant.
4. Results
Table 1 presents the demographic information. The participants included sixteen boys and five girls as well as their mothers.
Table 1.Demographic Information of Children with Intellectual Disability (n = 21)
| Variables | Mean ± Std. Deviation |
|---|---|
| Maternal education level (y) | 9.86 ± 6.643 |
| Education level of father (y) | 10.00 ± 6.403 |
| Child’s chronological age | 7.9833 ± 1.88072 |
| Child’s intellectual age | 4.4348 ± 0.58681 |
4.1. TOLD-P:3
According to the results of TOLD, all children with ID scored below 65 in the composite scores. The only exception was the composite score of semantics; in this regard, the average score for children with ID was above 70. The mean ± SD of language age for all subtests of TOLD-P:3 was 3;01 ± 0.04 except for Word Articulation which was 5.38 ± 2.30. For the sake of conciseness, the details on different score in the test are presented in Appendix 1.
4.2. Conversational Skills Rating Scale
Children’s scores in two different subscales of conversational skills rating scale are shown in Table 2. The means ± SDs for assertiveness and responsiveness were 3.64 ± 0.90 and 4.08 ± 0.87, respectively.
Table 2.The Percentiles of the Assertiveness and Responsiveness Subscales Scores
| Variables | Percentiles | ||||||
|---|---|---|---|---|---|---|---|
| 5 | 10 | 25 | 50 | 75 | 90 | 95 | |
| Responsiveness | 2.31 | 2.40 | 3.60 | 4.50 | 4.60 | 4.78 | 4.80 |
| Assertiveness | 2.40 | 2.41 | 2.53 | 4.33 | 4.47 | 4.60 | 4.66 |
4.3. Vineland Social Growth Scale
According to the SQ and out of all participants, seven participants (about 33%) scored at or above 100, while 14 ones (66.7%) scored below 100.
4.4. General Spontaneous Language Indices
As for different words, Mean ± SDs were 34 ± 18.72; MLU: 1.95 ± 0.88; TTR: 0.64 ± 0.16; the total number of complete sentences: 14.52 ± 13.35; and the percentage of complex sentences was: 19.71 ± 39.94.
4.5. Scio-conversational Analysis
Mean ± SD was 112.81 ± 27.16 for the number of turns; it was 54.81 ± 7.73 for the percentages of mothers’ turns and 45.19 ± 7.73 for the children’s turns. The difference between mothers’ portion and children’s portion was significant (P < 0.001).
The mean and standard deviation of children’s socio-conversational skills, according to the Fey’s model, was 27.34 ± 23.17 for assertiveness and it was 72.66 ± 23.17 for responsiveness. Tables 3 and 4 indicate the distribution of children and their mothers based on their socio-conversational behaviors during the interaction.
Table 3.The Percentiles of Children’s Communication Behaviors During Interaction
| Percentiles | |||||||
|---|---|---|---|---|---|---|---|
| 5 | 10 | 25 | 50 | 75 | 90 | 95 | |
| Assertiveness | 0.00 | 0.00 | 4.88 | 26.92 | 43.67 | 65.78 | 72.67 |
| Responsiveness | 27.33 | 34.22 | 56.34 | 73.08 | 95.12 | 100 | 100 |
Table 4.The Percentiles of Mothers’ Communication Behaviors During Interaction
| Percentiles | |||||||
|---|---|---|---|---|---|---|---|
| 5 | 10 | 25 | 50 | 75 | 90 | 95 | |
| Assertiveness | 52.65 | 59.96 | 66.90 | 91.07 | 98.08 | 100 | 100 |
| Responsiveness | 0.00 | 0.00 | 1.84 | 6.78 | 33.11 | 40.04 | 47.35 |
In Table 5, children are presented alongside mothers to show the possibility of relationship between mothers’ parenting styles and children’s role during the interactions.
Table 5.The Distribution of Children with ID and Their Mothers
| Parenting Style | Total | ||
|---|---|---|---|
| Authoritative Style with High Levels of Both Responsiveness and Demandingness | Authoritarian Style with Low Levels of Responsiveness But High Levels of Demandingness | ||
| Child’s role | |||
| Active conversationalist (+Assertiveness +Responsiveness) | 0 | 5 | 5 |
| Passive conversationalist (-Assertiveness +Responsiveness) | 0 | 14 | 14 |
| +Assertiveness -Responsiveness (Verbal non-communicator) | 2 | 0 | 2 |
| Total | 2 | 19 | 21 |
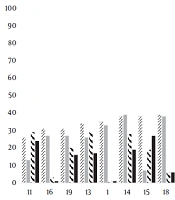
Analyzing the socio-conversational behaviors of the mothers revealed that only two mothers adopted authoritative style (high levels of both responsiveness and assertiveness; means ± SDs were equal to 44.77 ± 4.57 and 55.23 ± 4.57), and nineteen of them were authoritarian (low responsiveness and high demandingness; means ± SDs were equal to 12.69 ± 13.63 and 86.48 ± 13.47 in that order). Those two mothers adopting authoritative style had children who took the verbal non-communicator role during interactions. The children of the mothers with authoritarian style were divided asymmetrically into two different interactive roles: Passive and active conversationalists; Figure 2 is presented to clarify this concept.

Figure 2.
Mothers versus children communication behaviors
Investigating the relationship between conversational skills and common language indices produced different findings: Insignificant relationship between children’s socio-conversational behaviors and TTR, or number of different words, or percentage of simple utterances. The only positive significant relationship was found between MLU and assertiveness (r = 0.48, P = 0.027) (see Appendix 2 for more details).
5. Discussion
The present study evaluated the pragmatic skills of 21 children with ID who were students in special needs schools. The research team implemented a comprehensive set of assessment tools. The first level of evaluation indicated that all these students scored as “very-weak” in TOLD-P:3. According to the results from this test, their language age was comparable to the language skills of typical children at age three. This finding may have been attributed to the fact that children with ID lagged behind their typical peers in language skills (in present study, about one year based on their non-verbal mental age), a finding that was in line with findings reported by previous studies in English-speaking children with ID (35, 47-50). All previous studies have indicated that multiple developmental patterns for language skills could be found in children with ID, and that all of them are represented in different types of language delays (46, 49).
The socio-conversational analysis based on the Fey’s model indicated that two-thirds of children were “passive conversationalist”, five children were “active conversationalist”, and two of them were non-verbal communicators during interaction. Mar and Sall extracted the profiles of expressive communication skills in children and adolescence with severe to profound ID. They examined the basic forms of communication, communication intentions, social reciprocity, and the complexity of interaction, and reached to seven different forms of communication profiles (from simple reaction to complex interaction). The severity of intellectual disability in their study (severe versus profound) was a factor that may have explained the differences between communication profiles (51). In another study by Smith et al. (50), the pragmatic skills of 29 six-year-old children with Down Syndrome were assessed based on Children's Communication Checklist-2. Their participants showed impairments relative to the norms of this checklist. Their communication profiles included both strengths and weaknesses, but, taking into account all of their evaluations, they concluded that all of their participants had significantly pragmatic impairment by the age of six. Although major methodological differences may have been found between the present study and the given studies, the outcomes were extremely similar. Children with ID presented different ranges of communication skills assessed either by a questionnaire or by analyzing their interactions.
As discussed earlier in the introduction section, passiveness gives the child less opportunity to achieve all the advantages of social interaction. A vicious cycle is initiated and worsens with child’s language difficulties or their social maturity and quotient (52, 53). The SQ makes people more responsible. People, in addition to taking their own responsibility, become aware of the problems in their society, their surroundings, their workplace peers and subordinates, their country, and, then, their universe as well. The SQ helps people to interconnect their personal vision to the greater good of humanity. The above-mentioned two-thirds of children, along with their mothers, who failed to be highly assertive and responsive during interaction scored below average function in their social skills.
Mothers reported their children’s conversational skills through the Conversational Skills Rating Scale. Three mothers described their children as “no or infrequent pragmatic skills”, whereas the others described their children as “emerging pragmatic competence”. Those three children with “no or infrequent pragmatic skills” were “passive conversationalist” during interaction. Therefore, the mothers’ judgments about their children’s conversational skills may have been accurate. None of the children received scores above 4.8 to be considered as “well- developed” in pragmatic skills, particularly those children with “active conversationalist role”, which may have been attributable to their language difficulties. This finding was in line with the results reported by Girolametto and Salmani et al. who suggested that the assertiveness and responsiveness scores of children with language impairment, according to their parents, were less than the level devoted to the well-developed pragmatic skills (43, 54). The scores of those three children with “no or infrequent pragmatic skills” were comparable to the scores of typically developing children aged 12 - 24 months in Shakibi and Aslanifar’s study. It was recommended that the SLP for these three clients should focus first on the pragmatic skills and then, on other areas of language, including form and content, based on the Fey’s model.
In the current study, no control group with normal intelligence was included. Therefore, it was difficult to determine who affected the other - in other words, the language difficulties determined parents’ “authoritarian” style, or parents were responsible for children’s passive position. According to the previous studies such as Ghorbani et al., the dominant parenting style among Iranian mothers was authoritarian (55). However, recent studies such as Ashtari et al. and Khanipour et al. highlighted the existence of other parenting styles among Iranian mothers and confirmed the positive effects of such styles on children’s language skills (36, 38). Taking into account all language findings (TOLD-P3, language sample analysis, and general language indices) as well as the relationship between assertiveness and MLU, on the other hand, our participants lacked the required language abilities to lead the interaction, which may have explained the reason why parents used a particular style. They attempted to have more teaching behaviors than responsive acts. Vilaseca et al. analyzed the interactions between parents and their children with ID, and reported a range of valuable findings, including a significant positive relationship between mothers' teaching behaviors and children’s ages (56). Since our participants were in school age but had insufficient language skills, their mothers were likely intended to teach them the concepts during interaction and, therefore, avoided playing games or spending enjoyable time with them. As the result, it was not possible to directly attribute the children’s “discontented and withdrawn” position to parenting style or to attribute children’s “assertiveness and self-reliance” to others “authoritative” style.
5.1. Limitations
This study faced some limitations. First, there was not equal number of male and female participants, and, therefore, other studies may have reached different conversational skill profiles for these children. Second, only school children with non-specific ID who had language output were included in this study; therefore, the study results may have been generalized to other children with ID only with caution. Third, there was no control group without ID in our study; therefore, our data and comparison may not have been safely generalized to the general population.
5.2. Conclusions
In sum, a remarkable delay in language skills, especially conversational skills of children with non-specific ID, was found and highlighted. The most common parenting style was detected to be the controlling style; due to the limitations of our study, however, no definite conclusion was drawn concerning the causal relationship between parenting style and children’s language delays. Children with ID played different roles during interaction, but most of them were inclined to be “passive conversationalist”.