

1. Introduction
Calcifying tendonitis (CT) is defined as the deposition of hydroxyapatite within tendons. CT could affect different tendons, as the rotator cuff, Achilles, patella, forearm extensors, biceps brachi, and tibialis posterior tendons. The etiology is multifactorial and its pathophysiology is still unclear; degeneration plays and important role in CT. Literature described 3 stages with clinical/histological and radiological correlation: 1, Precalcification: tenocyte metaplasia/chondrocyte transformation; 2, Calcification: a. formative, b. resorptive (spontaneous resorption/phagocytosis); 3, Postcalcification: collagen remodeling/tendon repair. CT diagnosis is both clinical and radiological. Conservative treatment includes nonsteroidal anti-inflammatory drugs (NSAIDs), physiotherapy, electrotherapy (micro-waves, short-waves, transcutaneous electrical nerve stimulation (TENS), ultrasounds, iontophoresis, interferential, and pulsed electromagnetic therapy). Advanced treatment includes shock-waves, eco-guided aspiration, and arthroscopy (1-3).
Iontophoresis is a conservative, non-surgical technique that favors the penetration of transdermal substances/drugs through the skin with the help of electric current, based on physical-chemical properties of attraction and repulsion of charges. In the 1950s, Psaki and Carroll were the first to use acetic acid iontophoresis as an effective treatment for shoulder CT (4). However, there are controversial results on CT, and limited case reports on effectiveness in other tendons such as gluteus medium and minimum and Achilles’ tendons (5). To the best of authors` knowledge, there is no report on the effectiveness of acetic acid iontophoresis and ultrasound on bilateral calcifying tendonitis of Achilles’ tendons.
2. Case Presentation
The current study reports the case of a 57-year-old female with a 12-month experience of bilateral Achilles’ tendon pain that increased with walking and using tight shoes. She was a right-handed housewife, with no important antecedents. NSAIDs did not alleviate pain. She already went through physical therapies (laser and physiotherapy) without any success. Due to failure, she also went through bilateral shock wave therapy, but no alleviation was observed on pain or the calcification. Radiography showed bilateral insertional formative calcification on both Achilles’ tendons confirmed by ultrasound scan (Figures 1 and 2); 9.6 mm length in its longer axis, at the insertion of the left Achilles’ tendon, and 6.6 mm length on the right Achilles’ tendon. After 15 sessions of 5% acetic acid iontophoresis (2 mL, 4.7 mA × 10 minutes) and continuous ultrasound (1 W/cm2,1 MHz × 5 minutes) over the calcification area, pain decreased from 9/10 to 4/10 (left tendon) and from 5/10 to 0/10 (right tendon) on visual analogical scale (VAS). Calcification disappeared after treatment (from 6.6 to 0 mm) on the right tendon and decreased from 9.3 to 4.3 mm on the left tendon, after radiographic and ultrasound evaluation.

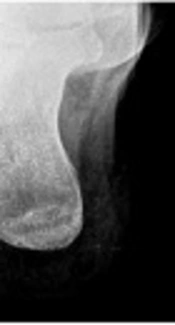
Before treatment: pain measured by VAS 9/10, calcification 9.3 mm evaluated by sonography (A) and radiography (C). After treatment pain measured by VAS 4/10, calcification 4.3 mm evaluated by sonography (B) and radiography (D).

Before treatment: pain measured by VAS 5/10, calcification 6.6 mm evaluated by sonography (A) and radiography (C). After treatment: pain measured by VAS 0/10, calcification 0 mm evaluated by sonography (B) and radiography (D).
The treatment protocol consisted of 2 mL of 5% acetic acid iontophoresis dropped into a gauze and placed onto the moistened cation electrode (negative electrode), covered by a 10 × 10 cm sponge, and it was directly put in contact with the ankle, next to Achilles insertion (Figure 3A). The Anion electrode (positive electrode) was placed 10 cm distal to the ankle, over the ventral part of the foot, covered by a moistened 10x10 cm sponge. Subsequently, continuous Ultrasound with an intensity of 1 W/cm2 and 1 MHz frequency was applied for 5 minutes at the insertion of the Achilles’ tendon on the affected ankle.
 are Dropped at the Cation Electrode (Negative Electrode), For Iontophoresis Treatment, a Galvanic Current at 4.7 mA Intensity Was Applied for 10 Minutes (B)")
Acetic Acid 5%, 2 mL in a Gauze (A) are Dropped at the Cation Electrode (Negative Electrode), For Iontophoresis Treatment, a Galvanic Current at 4.7 mA Intensity Was Applied for 10 Minutes (B)
To perform the treatment protocol, 2 European medical devices were used: 1, for Iontophoresis, ENDOMED 581 ID (Enraf Nonius® CE 0197; Salamanca, Spain) (Figure 3B); and 2, for ultrasound, SONOPULS 490 (Enraf Nonius® CE 0197; Salamanca, Spain).
3. Conclusion
The current case report confirmed that 5% acetic acid iontophoresis plus ultrasound was safe and effective to treat bilateral calcifying tendonitis of Achilles’ tendons.
