






1. Background
Nephrolithiasis is one of the most common complaints causing patients to refer to emergency wards. Renal stones may present a variety of clinical manifestations such as typical renal colic, a vague pain at the flank, or an unexplained urinary tract infection. Thus, accurate diagnosis of renal stones is important for proper treatment. Many diagnostic modalities are used to identify renal stones such as plain radiographs, ultrasonography, and computed tomography (CT) (1-4). CT is the gold standard for the detection of urolithiasis; however, it may have some disadvantages and limitations. CT scan uses x-rays for imaging of the tissues of interest, and radiation safety and patient dose are major concerns regarding this imaging technique. CT has limited application in pregnant patients, is costly, and is not available in all emergency wards. Moreover, patients with urolithiasis may need to be followed up; and using CT scan for follow up purposes is not currently recommended (5, 6).
Ultrasonography (US) is a safe, cost-efficient, and fast modality which is used in for imaging and diagnosing pathologies. Although the accuracy of sonography in diagnosing lithiasis is inferior to that of a non-contrast CT image, especially in smaller stones, there is a tendency to use US instead of CT in patients with a probable diagnosis of nephrolithiasis. Urolithiasis is seen as echogenic structures with posterior shadowing in US. However, smaller lithiasis (smaller than 5 mm) may be without posterior shadowing and have similar echogenicity to surrounding structures of the kidney, vessel walls, or renal sinus fat, causing failure in the detection of these stones (7).
The twinkling artifact, also known as the color comet tail artifact, is a focus of alternating colors on Doppler sonography behind a reflective object (such as calculi), which gives the appearance of turbulent blood flow. The signal is persistent even if the pulse repetition frequency (PRF) is adjusted to higher levels and does not show any wave at pulse wave mode. It was first described by Rahmouni et al. at 1996 for the detection of kidney stones (8-12).
2. Objectives
In this study, we aimed to investigate the accuracy of sonographic twinkling artifact sign in the detection of CT-confirmed renal stones smaller than 4 mm.
3. Methods
3.1. Patients
This study was performed on patients with a probable diagnosis of urolithiasis referred to the CT scan ward of a tertiary medical-educational center during April to September 2019. Patients with renal stones smaller than 4 mm in diameter on CT scans were included. Patients with renal stones greater than 4 mm in diameter and patients who were being treated with Indinavir were excluded from the study. Overall, 110 patients were considered for inclusion, of which 99 patients had kidney stones confirmed on CT scan. CT scan was considered as the gold standard.
3.2. CT Scan
All patients underwent unenhanced helical CT examination using a Somatom Plus 4 unit (Siemens, Germany). Axial scans were taken from the top of the kidneys to the base of the bladder with a 5-mm collimation, a 2:1 pitch, 120 kVp, 280 mAs, and reconstruction at 2.5-mm intervals.
An independent, experienced radiologist with at least 15 years of experience reviewed each CT examination for the presence of stones in the kidneys at a workstation capable of reconstruction reformatting. Patients having renal stones smaller than 4 mm were referred to the sonography ward in order to investigate US findings.
3.3. Ultrasonography Study
Within 24 hours of CT imaging, US study of the abdomen was performed by a radiologist with 10 years of experience who was blind to the patient’s CT scan findings, using a Philips iU22 unit (Philips Healthcare Andover, Mass) equipped with a 2 - 5 MHz convex probe.
Both gray scale and color Doppler ultrasonography exams were performed in all patients. On the gray scale, US, presence of stone, its location and size, and presence of posterior shadowing were investigated. Color Doppler ultrasonography was performed using a red and blue color map to detect the twinkling artifact. The color window size was adjusted to cover the whole renal sinus. For renal stones, the pulse repetition frequency (PRF) was set just above 60 cm/sec to eliminate color flow signals from renal blood flow. Whenever a twinkling sign was present, a pulse wave was obtained to exclude arterial or venous flow.
Statistical analysis: Statistical analysis was performed by SPSS (SPSS Inc., Chicago, IL). Quantitative data was presented as mean ± standard deviation. A paired T-test was used to compare the CT and Sonography quantitative values. McNemar’s test was used to compare qualitative values. P value less than 0.05 was considered statistically significant. In order to evaluate the accuracy of twinkling artifact in diagnosing small renal stones, its sensitivity, specificity, positive predictive value, and negative predictive value was measured. Sample size calculation was performed using the open source software R (R Foundation, Auckland, New Zealand)
3.4. Ethical Considerations
This study was conducted after being approved by the local Ethical board of the medical center in which it was performed. The whole process was explained to the patients before entering the study, and the patients signed informed consent notes. Patients who had accepted to participate in the study were included. All information of patients, including the demographical data and CT scan and US findings, remained undisclosed to any third party.
4. Results
In this study, during 6 months from April 2019 to September 2019, of all patients referred to the CT scan ward of a tertiary medical center with a diagnosis of urolithiasis, 110 patients were initially considered for inclusion, of which 99 had nephrolithiasis proven by CT imaging. The patients’ age ranged from 15 to 78 years old, with a mean of 38.7±16.24 years. 84 patients (85%) were males.
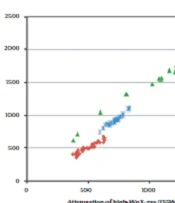
Of the 99 patients with confirmed lithiasis in non-contrast CT scans, renal stones were detected as echogenic structures in 91 patients (91.91%) with abdominal gray scale sonography. In 8 patients, no evidence of lithiasis was observed on gray scale sonography. There was posterior shadowing behind the renal stone (echogenic structure) in 70 patients (70.7%).
Table 1 shows the detected renal stones’ site on both CT scan and US.
Table 1.Renal Stone Sites Found on CT Scan and US
| Kidneys | Poles of Kidneys | ||||
|---|---|---|---|---|---|
| Right Kidney | Left Kidney | Upper Pole | Middle Pole | Lower Pole | |
| CT scan (99 stones) | 40 (40.4%) | 59 (59.6%) | 19 (19.2%) | 46 (46.5%) | 34 (34.3%) |
| US (91 stones) | 37 (40.7%) | 54 (59.3%) | 17 (18.7%) | 41 (45.1%) | 33 (36.3%) |
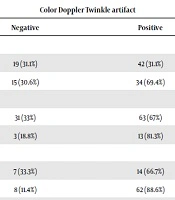
On color Doppler US, there was a twinkling artifact in 76 of 99 patients with confirmed renal stones on non-contrast CT scan. Sensitivity, specificity, positive predictive value, and negative predictive value for the twinkling artifact in detecting renal stones were 76.8%, 100%, 100%, and 32.4%, respectively. The correlation between the presence of twinkling artifact and the presence of stones was statistically significant (P value < 0.0001). Results did not show any correlation between twinkling artifact and age, gender, side of the involved kidney, or the involved pole of the kidney. However, there was a significant correlation between US twinkling artifact and posterior shadowing at US.
Table 2.Doppler Findings in Relation to the Characteristics of Patients.
| Factor | Color Doppler Twinkle artifact | P | |
|---|---|---|---|
| Negative | Positive | ||
| Age | 0.952 | ||
| Less than 40 | 19 (31.1%) | 42 (31.1%) | |
| More than 40 | 15 (30.6%) | 34 (69.4%) | |
| Sex | 0.255 | ||
| Male | 31 (33%) | 63 (67%) | |
| Female | 3 (18.8%) | 13 (81.3%) | |
| Posterior shadowing | 0.038 | ||
| Yes | 7 (33.3%) | 14 (66.7%) | |
| No | 8 (11.4%) | 62 (88.6%) | |
| Kidney side | 0.887 | ||
| Left | 14 (23.7%) | 45 (76.3%) | |
| Right | 9 (22.5%) | 31 (77.5%) | |
| Location in kidney | 0.503 | ||
| Upper | 3 (15.8%) | 16 (84.2%) | |
| Middle | 13 (28.3%) | 66 (71.7%) | |
| Lower | 7 (20.6%) | 27 (79.4%) | |
5. Discussion
Our study was conducted on 99 patients from all patients who were referred to the CT scan ward of a tertiary medical, educational center with active nephrology and urology wards. Patients had a CT scan prior to inclusion, and those with existing urolithiasis were included. US was performed on the study population in order to investigate renal stones and the presence of posterior shadowing and twinkling artifact. The results of our study showed that the twinkling artifact on color Doppler US is significantly correlated with the presence of renal stones and posterior shadowing. The twinkling artifact has a sensitivity of 76.8%, specificity of 100%, the positive predictive value of 100%, and a negative predictive value of 32.4% in detecting renal stones.
In a similar study carried out in Romania by Gliga et al. on 113 patients; the results showed that the sensitivity, specificity, positive predictive value and negative predictive value of twinkling artifact in detecting renal stones smaller than 5 mm were 99.12%, 90.91%, 99.12%, and 90.91% respectively, which are similar to our findings (17).
In another study by Mitterberger et al. performed in Austria in 2009, 77 urinary tract stones in 41 patients were included. Their results indicated that twinkling artifact on color Doppler US is significantly correlated with the presence of urolithiasis. Interestingly, their findings revealed that using twinkling artifact in color Doppler US is more accurate than the presence of posterior shadowing for the detection of urolithiasis (97% vs. 66%) (7).
The study performed by Masch et al. on 85 patients revealed that isolated sonographic twinkling artifact has a sensitivity of 78%, the specificity of 40%, and positive likelihood ratio of 1.30 in detecting renal calculus. It was also declared that for the detection of calculi, the specificity and positive likelihood ratio of this US artifact increase if it is used in combination with posterior shadowing sign and presence of an echogenic focus (18). This study reported a considerably lower sensitivity compared to other studies. This could be because of differences in operators’ skill and the imaging protocols which were performed. Importantly, the blinding of operators seems an issue which is not discussed in such studies.
Another study by Dillman et al. examined the diagnostic accuracy of the twinkling artifact. In this study, the sensitivity and positive predictive value of twinkling artifact in detecting renal stone were lower (55% and 78%, respectively) compared to our study. The true-positive and false-positive rate of this artifact were 49% and 51%, respectively (19). The differences between results of the two studies can be explained by the difference in the imaging protocols, as Dillman et al. only used Doppler imaging. However, in our study, the radiologist was able to also use gray scale imaging. Sonrensen et al. studied 32 stone in 18 kidneys and found that twinkling artifact has a lower sensitivity, specificity, positive predictive value, and negative predictive value compared to other previously reported studies (56%, 74%, 62%, and 68% respectively). Their findings are inconsistent with our results. This inconsistency could be due to the small sample size of the current study (6).
Winkel et al. studied 105 patients with renal stones in Denmark and showed that twinkling artifact was present in 74% of renal stones detected on B-mode US. For detecting urolithiasis, gray scale and color Doppler US in combination had a sensitivity, specificity, positive predictive value, and negative predictive value of 55%, 99%, 67%, and 98%, respectively.
The difference between the findings of these studies may indeed reflect the different skill sets of operators. It may also be attributed to the characteristics of the stones being studied. In the present study, we found that no factor affected the accuracy of the twinkling artifact. However, our sample size was limited, and not all possible characteristics were included in the first place. Other studies also face the same limitation, with some studied even completely neglecting the anatomical location of the stones. We also don’t know the exact effect of the chemical composition of the stone on the aforementioned imaging findings, and none of the studies mentioned above have neither considered this factor.
By considering all these explanations and the fact that US is cost-efficient, without harmful radiation, and readily available, more emphasis can be put on US in diagnosing nephrolithiasis. Moreover, supplementation of Doppler imaging may eliminate the necessity for performing a CT scan.