





1. Background
End-stage kidney disease (ESKD) patients undergoing hemodialysis suffer from multiple comorbidities, including cardiovascular disorders. The ESKD patients frequently suffer from sleep disorders, pain, and dysfunctional sexual life (1, 2). Lack of control over their own lives, anxiety, and panic disorder are other problems affecting the health-related quality of life (HRQOL) in patients receiving hemodialysis (2). HRQOL in several domains is studied for maintenance hemodialysis patients. Patients with ESKD surviving on dialysis generally have low quality of life. Focused care among these patient populations results in improved physical, emotional, and social performance, leading to higher life quality experience among the concerned patients (3). However, the association between increasing HRQOL and decreased cardiovascular risk among ESKD patients on maintenance hemodialysis has not been detected yet.
The kidney disease population has about 20 times higher susceptibility to cardiovascular disease than the healthy population. Cardiovascular disease is the leading cause of death due to secondary complications in patients suffering from kidney diseases (4). Advancements in clinical practice have improved treatment in dialysis; however, the frequency of cardiovascular mortality in these patients is still high. The different cardiovascular implications of ESKD include left ventricular hypertrophy, myocardial fibrosis, microvascular disease, accelerated atherosclerosis, arteriosclerosis, and myocardial ischemia (5). Hemodialysis may lead to hemodynamic instability and the initiation of systemic inflammation as well. Apart from the aforementioned risks, the other determinants are chronic volume overload, anemia, inflammation, oxidative stress, kidney disease, and mineral bone disorder (6).
Mineral metabolism abnormalities are common in kidney failure patients and are associated with an increased risk of cardiovascular events. However, few studies have examined the effects of phosphorus and calcium phosphate (CaP) product on outcomes in individuals with CKD stages 3 - 4. The Modification of diet in renal disease study evaluated the connection between serum phosphorus level and CaP product with all-cause and cardiovascular disease (CVD) morbidity in 840 patients. After adjusting for glomerular filtration rate, the serum phosphorus level and CaP product were not statistically associated with all-cause or cardiovascular disease mortality. However, the CaP product is linked to predicting mortality risk in dialysis patients with ESKD. Furthermore, a high CaP product was linked to a higher 1-year mortality rate (7, 8).
It is essential to understand if kidney disease-specific HRQOL can be correlated with one of the specific markers of cardiovascular risk, i.e., CaP product. HRQOL might have an association with morbidity and mortality levels in some specific diseases, but not in all diseases. Accordingly, it is essential to detect whether HRQOL influences treatment decisions and whether it has a correlation with the CaP products.
2. Methods
The present study used a cross-sectional design to explore the correlation between HRQOL and the CaP product. The HRQOL survey was filled by the researcher using a standard tool. The research population encompassed all patients undergoing hemodialysis at a single medical center as part of their ESKD management. In this population-based study, all hemodialysis patients meeting our inclusion and exclusion criteria took part. Data from the patient population was collected in February and March 2021.
2.1. Inclusion Criteria
Inclusion criteria is as follow: (1) 18 - 85 years of age; (2) patients on maintenance hemodialysis for above three months; and (3) patients willing to sign the informed consent.
2.2. Exclusion Criteria
Exclusion criteria is as follow: (1) patients on hemodialysis for acute kidney injury; (2) patients on other forms of hemodialysis or peritoneal dialysis.
The study was conducted at the hemodialysis ward of the hospital affiliated with Gulf Medical University. It is one of the largest hemodialysis units in the United Arab Emirates in the private sector, with ten beds and above 50 ESKD patients on maintenance hemodialysis. The 350-bed hospital affiliated with the Thumbay University is a private academic hospital in the United Arab Emirates.
2.3. Criteria for Data Determination
The researcher filled kidney disease and quality of life (KDQOL-36) during an interview with hemodialysis patients. KDQOL-36 has the short form (SF)-12adressing kidney-specific domains. It was filled at once for all patients for all 36 items (9):
● SF-12 physical composite (items 1, 2, 3, 4, 5, 8, 10, 12);
● SF-12 mental composite (items 1, 6, 7, 9, 11, 12);
● Kidney specific domains;
● Burden of kidney disease (Items 13 - 16);
● Symptom/problem list (items 17 - 28);
● Effects of kidney disease (items 29 - 36).
Each item is converted out of 100 before taking the mean HRQOL per domain. Higher scores indicate better HRQOL. Some items should be reversely scored according to the instructional manual of KDQOL-36:
● Item 1, reverse (100-75-50-25-0);
● Items 2 - 3, regular (0-50-100);
● Items 4 - 5, regular (0-100);
● Items 6 - 7, regular (0-100);
● Items 8, reverse (100-75-50-25-0);
● Items 9 - 11, reverse (100-80-60-40-20-0);
● Items 12, regular (0-25-50-75-100);
● Items 13 - 16, regular (0-25-50-75-100);
● Items 17 - 28, reverse (100-75-50-25-0); and
● Items 29 - 36, reverse (100-75-50-25-0) (9).
2.4. Data Analysis
Spearman’s correlation coefficient (rs) indicated strongly high correlation (0.90 - 1.00), high correlation (0.70 - 0.90), moderate correlation (0.50 - 0.70), low correlation (0.30 - 0.50), negligible correlation (0.00 - 0.30) (10).
Regarding the KDIGO guidelines, CaP product > 55 mg/dL is set as a cardiovascular risk in the ESKD patients. CaP product is calculated by multiplying calcium and phosphate. In this regard, total calcium is concerned, and calcium binds to albumin. In patients with low levels of blood albumin, the following formula is used to correct calcium level: Corrected total calcium (mg/dL) = Total calcium (mg/dL) + 0.8 × [4 - Serum albumin (g/dL)] (8).
The investigators filled these instruments in discussion with patients undergoing hemodialysis. There were frequent meetings among investigators to go through the collected data to validate it. The confidentiality of the patients’ information was also considered in this study. The institutional review board approval was obtained before data collection.
3. Results
The HRQOL and demographic details of 41 ESKD patients were collected from above 50 patients regarding the inclusion and exclusion criteria. The patients’ mean age was 46 (range 40 - 59) years. A majority of the participants were males (73%), 95% of the participants were married, 44% of the patients were employed, 42% of the participants, including housewives, were unemployed, and 14% of the participants were retired. About half of the participants (56%) were university graduates. Concerning primary diseases, 95% and 66% of the participants had hypertension and diabetes, respectively. No patient reported alcohol use, and few cases reported no smoking habit. Only 21% of the patients had normal body mass index (BMI), and the others were obese (34%) and overweight (45%). Dry weight was used to calculate BMI.
Moreover, 85% of the patients reported paying through charity, 10% of the cases paid out-of-pocket, and 5% of the participants had their health insurance coverage. A majority of the patients (68%) had three sessions per week, while 32% of the participants had two sessions per week. UAE has a high expatriate population. Regarding the patients’ nationality, 51% of the study population were from other Arab countries, and there were 2% from UAE, and 46% from different Asian countries (primarily South Asian). All patients answered all 36 questions of the HRQOL survey. The patients rated their overall impression of health as excellent (14%), very good (24%), good (31%), fair (29%), and poor (2%).
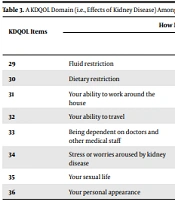
The mean score (58%) of the SF-12 physical composite was lower than the mental composite (70%). Among the kidney-specific domains, the highest HRQOL was with symptom/problem list (71%) followed by effects on kidney disease (63%) and burden of kidney disease (40%), respectively. Tables 1 - 3 show kidney-specific domains, including burden of kidney disease, symptom/problem list, and effects of kidney disease.
| KDQOL Items | How True or False Is Each of the Following Statements for You?41 Responses | |||||
|---|---|---|---|---|---|---|
| Questions | Definitely True | Mostly True | Don’t Know | Mostly False | Definitely False | |
| 13 | My kidney disease interferes too much with my life | 19 (46.3) | 10 (24.4) | 6 (14.6) | 2 (4.9) | 4 (9.8) |
| 14 | Too much of my time is spent with my kidney disease | 25 (61) | 7 (17.1) | 4 (9.8) | 2 (4.9) | 3 (7.3) |
| 15 | I feel frustrated dealing with my kidney disease | 11 (26.8) | 11 (26.8) | 8 (19.5) | 7 (17.1) | 4 (9.8) |
| 16 | I feel like a burden on my family | 4 (9.8) | 9 (22) | 4 (9.8) | 4 (9.8) | 20 (48.8) |
A KDQOL Domain (i.e., Burden of Kidney Disease) Among Hemodialysis Patients a
| KDQOL Items | During the Past Four Weeks, to What Extent Were You Bothered by Each of the Following Symptoms? | |||||
|---|---|---|---|---|---|---|
| Sign/Symptom | Not at All Bothered | Somewhat Bothered | Moderately Bothered | Highly Bothered | Extremely Bothered | |
| 17 | Soreness in your muscles | 11 (26.8) | 9 (22) | 9 (22) | 9 (22) | 3 (7.3) |
| 18 | Chest pain | 31 (75.6) | 2 (4.9) | 2 (4.9) | 6 (14.6) | 0 (0) |
| 19 | Cramps | 11 (26.8) | 13 (31.7) | 6 (14.6) | 5 (12.2) | 6 (14.6) |
| 20 | Itchy skin | 20 (48.8) | 10 (24.4) | 2 (4.9) | 4 (9.8) | 5 (12.2) |
| 21 | Dry skin | 15 (36.6) | 10 (24.4) | 5 (12.2) | 3 (7.3) | 8 (19.5) |
| 22 | Shortness of breath | 25 (61) | 6 (14.6) | 4 (9.8) | 6 (14.6) | 2 (4.9) |
| 23 | Faintness or dizziness | 17 (41.5) | 10 (24.4) | 8 (19.5) | 5 (12.2) | 1 (2.4) |
| 24 | Lack of appetite | 20 (48.8) | 9 22) | 7 (17.1) | 3 (7.3) | 2 (4.9) |
| 25 | Washed out or drained | 14 34.1) | 8 (19.5) | 9 (22) | 6 (14.6) | 6 (14.6) |
| 26 | Numbness in hands or feet | 10 (24.4) | 9 (22) | 10 (24.4) | 11 (26.8) | 1 (2.4) |
| 27 | Nausea or upset stomach | 22 (53.7) | 12 (29.3) | 1 (2.4) | 5 (12.2) | 1 (2.4) |
| 28 | Problem with the access site | 20 (48.8) | 6 (14.6) | 5 (12.2) | 7 (17.1) | 3 (7.3) |
A KDQOL Domain (i.e., Symptom/Problem List) Among Hemodialysis Patients a
| KDQOL Items | How Much Does Kidney Disease Bother You in Each of the Following Areas? | |||||
|---|---|---|---|---|---|---|
| Not at All Bothered | Somewhat Bothered | Moderately Bothered | Highly Bothered | Extremely Bothered | ||
| 29 | Fluid restriction | 16 (39) | 7 (17.1) | 8 (19.5) | 6 (14.6) | 2 (4.9) |
| 30 | Dietary restriction | 17 (41.5) | 13 (31.7) | 3 (7.3) | 5 (12.2) | 3 (7.3) |
| 31 | Your ability to work around the house | 6 (14.6) | 10 (24.4) | 11 (26.8) | 6 (14.6) | 8 (19.5) |
| 32 | Your ability to travel | 8 (19.5) | 8 (19.5) | 4 (9.8) | 6 (14.6) | 15 (36.6) |
| 33 | Being dependent on doctors and other medical staff | 13 (31.7) | 14 (34.1) | 7 (17.1) | 2 (4.9) | 5 (12.2) |
| 34 | Stress or worries aroused by kidney disease | 20 (48.8) | 7 (17.1) | 6 (14.6) | 4 (9.8) | 4 (9.8) |
| 35 | Your sexual life | 13 (31.7) | 9 (22) | 13 (31.7) | 2 (4.9) | 4 (9.8) |
| 36 | Your personal appearance | 11 (26.8) | 9 (22) | 10 (24.4) | 10 24.4) | 1 (2.4) |
A KDQOL Domain (i.e., Effects of Kidney Disease) Among Hemodialysis Patients a
The corrected CaP product was calculated for 32 patients from the available laboratory tests. Their average CaP product was 42 ± 15. In this study, we observed CaP product > 55 mg/dL for 28% (approximately half of them were just in the border of CaP product = 55 - 56 mg/dL), 45 - 54.9 mg/dL for 13%, and < 45 mg/dL for 59% of the patients. Moreover, CaP product > 55 mg/dL is considered a cardiovascular risk, which needs to be confirmed with computerized tomography.
Spearman's rho was calculated for SF-12 physical composite, mental composite, the burden of kidney disease, symptoms/problem list, effects of kidney disease, and categorized CaP product. A low negative correlation was noticed between the burden of kidney disease and the corrected CaP product (rs = -0.439, P = 0.032). The correlation between symptom/problem list and corrected CaP product (rs = -0.431, P = 0.035) was not strong as well. Furthermore, SF-12 physical composite, mental composite, and the effects of kidney disease revealed no significant relationship with CaP product (Table 4).
| Spearman's rho (rs) | SF Physical | SF Mental | Burden of Kidney Disease (Items 13 - 16) | Symptom/Problem List (Items 17 - 28) | Effects of Kidney Disease (Items 29 - 36) | CaP Product | Corrected CaP Product |
|---|---|---|---|---|---|---|---|
| SF-12 physical composite | |||||||
| Correlation coefficient | 1.000 | 0.217 | 0.317 a | 0.487 b | 0.477 b | 0.192 | 0.119 |
| P-value | - | 0.173 | 0.044 | 0.001 | 0.002 | 0.292 | 0.581 |
| N | 41 | 41 | 41 | 41 | 41 | 32 | 24 |
| SF-12 metal composite | |||||||
| Correlation coefficient | 0.217 | 1.000 | 0.389 a | 0.277 | 0.328 a | -0.101 | -0.266 |
| P-value | 0.173 | - | 0.012 | 0.080 | 0.036 | 0.583 | 0.209 |
| N | 41 | 41 | 41 | 41 | 41 | 32 | 24 |
| Burden of kidney disease | |||||||
| Correlation coefficient | 0.317 a | 0.389 a | 1.000 | 0.584 b | 0.323 a | -0.511 b | -0.439 a |
| P-value | 0.044 | 0.012 | - | 0.000 | 0.039 | 0.003 | 0.032 |
| N | 41 | 41 | 41 | 41 | 41 | 32 | 24 |
| Symptom/problem list | |||||||
| Correlation coefficient | 0.487 b | 0.277 | 0.584 b | 1.000 | 0.659 b | -0.187 | -0.431 a |
| P-value | 0.001 | 0.080 | 0.000 | - | 0.000 | 0.306 | 0.035 |
| N | 41 | 41 | 41 | 41 | 41 | 32 | 24 |
| Effects of kidney disease | |||||||
| Correlation coefficient | 0.477 b | 0.328 a | 0.323 a | 0.659 b | 1.000 | -0.028 | -0.195 |
| P-value | 0.002 | 0.036 | 0.039 | 0.000 | - | 0.878 | 0.360 |
| N | 41 | 41 | 41 | 41 | 41 | 32 | 24 |
| CaP product | |||||||
| Correlation coefficient | 0.192 | -0.101 | -0.511 b | -0.187 | -0.028 | 1.000 | 0.991 b |
| P-value | 0.292 | 0.583 | 0.003 | 0.306 | 0.878 | - | 0.000 |
| N | 32 | 32 | 32 | 32 | 32 | 32 | 24 |
| Corrected CaP product | |||||||
| Correlation coefficient | 0.119 | -0.266 | -0.439 a | -0.431 a | -0.195 | 0.991 b | 1.000 |
| P-value | 0.581 | 0.209 | 0.032 | 0.035 | 0.360 | 0.000 | - |
| N | 24 | 24 | 24 | 24 | 24 | 24 | 24 |
Correlation Between HRQOL Domains and CaP Product
4. Discussion
A majority of the research population were well-dialyzed three times a week using charity payments. Some patients received dialysis twice a week as they perceived hemodialysis a stressful process. The HRQOL of patients on hemodialysis is regularly affected by their treatment (11, 12). Few participants had health insurance covering all medication and necessary laboratory tests. Charity mostly pays for dialysis; however, there are limited funds for other necessary costs. The rest of the cost is out-of-pocket for the patients. Financial difficulties for many participants impeded them to receive the best care.
The present study showed physical composite scores lower than the mental composite scores as found in the dialysis outcomes and practice patterns study (DOPPS). A cross-sectional analysis of the DOPPS in five European countries, Japan, and the USA, showed relatively higher physical composite scores compared to the mental composite scores (13). Similar to the DOPPS study, the present study also showed lower scores for the burden, followed by effects, and an even better symptom/problem list (13).
While patients' lives were highly affected by their kidney disease and they were spending much time on their care, they were not totally frustrated about it. They had less strong feeling about being a burden to their families. While the patients were less bothered with their signs/symptoms, numbness in hands or feet, soreness in muscles, drained, cramps, and dry skin were relatively bothering. Considering the effects of kidney disease, they were relatively bothered with their ability to travel, work around the house, sexual life, and personal appearance.
ESKD and maintenance hemodialysis affect an individual's physical, mental, emotional, and social activities (14). The main effect on HRQOL in patients receiving hemodialysis was their inability to continue work regularly. The frequency of hemodialysis is associated with unemployment status. Affordability issues decrease the frequency of hemodialysis (15). The frequent measurement of HRQOL could be laborious. Following up on focused symptoms could complement the HRQOL data, especially if it is identified as an area of improvement in patient care (16). The use of short forms in measuring patient-reported outcomes in routine practice shall improve communication and shared decision-making among healthcare professionals and patients (17).
Patients with ESKD often experience complex cardiovascular system functional changes (6, 18). The calcium and phosphorus metabolism alters as GFR decreases by < 60-mL/min. The calcium deposition of arteries leads to high pulse waves and increased cardiac afterload, resulting in hemodynamic alterations (7, 19). Abnormal calcium and phosphorus metabolism can enhance arterial stiffness and increase the likelihood of atherogenesis, a severe form of cardiovascular disease (20). Hyperphosphatemia and increased levels of CaP product act as contributors to cardiovascular disease risk in ESKD. The consequences of hyperphosphatemia include the development and progression of hyperparathyroidism and metastatic calcification, mediating the substantial mortality observed in patients with kidney diseases (21, 22).
Clinical data among hospitalized patients (not necessarily ESKD), on the other hand, are not abundant. The present study aimed to detect the relationship between admission CaP product and one-year mortality in hospitalized patients. To this end, all adult patients admitted to a tertiary referral hospital were analyzed during 2009 - 2013. Patients were included if phosphate measurements and serum calcium were obtained 24 hours after hospital admission. Admission calcium-phosphate product (calcium × phosphate) was stratified into six groups based on its distribution: < 21, 21- < 27, 27- < 33, 33- < 39, 39- < 45, and ≥ 45 mg2/dL2. A multivariate cox proportional hazard analysis was used to find the relationship between admission CaP product and one-year mortality using a CaP product of 33 - 39 mg2/dL2 as the reference group. A high CaP product in hospitalized patients was linked to a higher 1-year mortality rate (23).
The study has limitations, including the exploratory nature of the study and a limited sample size. Conclusive evidence can be generated only by further studies using larger sample sizes to test the hypothesis. HRQOL is not the only factor correlated with cardiovascular risk. This point needs to be further addressed.
4.1. Conclusions
HRQOL needs to be monitored and improved according to the results of different domains. Physical composite and burden of kidney disease also need further attention in managing HRQOL. The CaP product was well managed in most patients for whom the laboratory data were available. Some patients need additional treatment to control their CaP product as a cardiovascular risk minimization effort. The correlation between KDQOL domains and CaP product was not significant. HRQOL in patients undergoing maintenance hemodialysis may not be associated with CaP products. Further studies are also recommended to modify the HRQOL measures to detect correlations with cardiovascular risks.
