

1. Background
Chronic kidney disease (CKD) is one of the major health challenges (1). It is a progressive and irreversible disorder that eventually leads to uremia (2). CKD is one of the diseases affecting individuals’ quality of life (QOL) (3). Today, 2 - 3% of the world's population suffers from chronic renal failure (CRF) (4). The annual growth of 5 - 6% in the number of CRF patients makes this disease one of the main concerns in any country (5). In our country, the growth of new cases of CKD is 22.6% per year; hence, about 4000 new patients are annually added to the number of CRF patients (6). The importance of this disease is such that in the report on the burden of this disease in 2016, it was considered one of the ten leading causes of death, accounting for 9300 deaths per year. CKD has also been the main cause of death in Iran (7). One of the most common invasive treatments for CKD is hemodialysis (8). About 90% of CRF patients undergo hemodialysis, and 92% of dialysis patients prefer this treatment (9). Although hemodialysis increases CRF patients’ life expectancy, it also arouses many problems (10). Compared to heart failure, diabetes, and other chronic diseases, hemodialysis significantly increases total costs (11), adversely affects patients' mental imagery, and further reduces QOL in social, financial, physical, and psychological dimensions (12). Several definitions have been proposed for QOL; the term ’ QOL’ is inherently ambiguous, as it can refer both to the experience an individual has of one’s life and to the living conditions in which individuals find themselves (13). The World Health Organization (WHO) defines this term as an individual's perception of the current situation in terms of the culture in which one lives and the relationship of his/her perceptions with his/her goals, expectations, standards, and priorities (14). Over the past two decades, interest in evaluating and improving QOL in patients with chronic diseases has dramatically increased; hence, improving such patients’ daily functioning and QOL has become a goal (15). The QOL assessment helps to solve patients' problems more deeply (16). Recent clinical trials have revealed that QOL can be considered an indicator of the quality of health care and a part of a disease treatment plan; hence, the QOL measurement in chronic diseases can provide caregivers with more information about patients’ health and illness status and can be a useful guide to improve the quality of care (17). Accordingly, monitoring QOL is the best tool to assess the health level of hemodialysis patients and the response of these patients to treatment and care methods (18).
2. Objectives
Due to the increasing incidence and prevalence of CRF and given the significant effects of this disease on all aspects of individuals’ lives, and different meanings of QOL in different cultures, this study aimed to assess QOL and its determinants in hemodialysis patients in the dialysis centers in East Azerbaijan Province.
3. Methods
The present study was a descriptive-analytical, cross-sectional study on 200 hemodialysis patients referred to the Samintab Dialysis Center in Maragheh and the hemodialysis wards of Imam Reza, Sina, and Pediatrics Educational Hospitals, and Amir Al-Momenin, Mahallati, Shams, and 22 Bahman private hospitals in Tabriz in 2021. The sample size was calculated regarding the average of one ratio. The samples were included in the study using the stratified random sampling method. Inclusion criteria were as follows: Patients aged above 18 years, willingness to participate in the research, six months having passed from the start of hemodialysis, ability to participate interviews, and no history of hospitalization due to illness or other complications during the last six months. Patients with peritoneal dialysis and cases of death and kidney transplantation during the study period were excluded. Before completing the questionnaires, the research objectives were explained to the patients, and the questionnaires were completed after obtaining their informed consent. The data collection instruments were a demographic information checklist and the SF-36 Quality of Life Questionnaire. Demographic characteristics were age, gender, marital status, weight, height, level of education, quality information on dialysis (time to start dialysis, number of dialysis sessions, and duration of dialysis), and concomitant diseases (e.g., diabetes and hypertension). The questionnaires were completed by a trained questioner working in the dialysis ward. The QOL questionnaire consists of 36 items in two dimensions (physical and psychological) with eight scales (physical, physical functioning, physical pain, general health and energy, social functioning, emotional role, and mental health). The QOL questionnaire scores range from 0 to 100. The standardization of the SF-36 questionnaire was approved by Montazeri et al. The reliability coefficient of the seven scales was 77 - 95%, and it was 65% for the energy scale and vitality (19). The patients were classified into three groups in terms of QOL and their scores: Desirable (≥ 75), somewhat desirable or moderate (75 - 25), and undesirable (< 25) (20).
The collected data were coded and analyzed with SPSS software version 25. In descriptive statistics, frequency, mean, and standard deviation were used, and Spearman’s, Kruskal-Wallis, and Mann-Whitney U tests were used in analytical statistics.
To observe the ethical principles in research, all phases of the study were conducted following the approval of the Ethics Committees of the Maragheh University of Medical Sciences (Code: IR.MARAGHEHPHC.REC.1397.016) and the Tabriz University of Medical Sciences. Before presenting the questionnaire to the patients, the research objectives were explained to them. The participation in this study was voluntary, and the patients were ensured of the confidentiality of their information.
4. Results
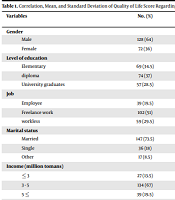
In this study, 64% of patients were male, and 36% were female. The mean age of hemodialysis patients was 49.4 ± 13.8 years in men and 42.7 ± 10.9 years in women. The patients' mean weight was 63.7 ± 1.9 kg, and the mean height was 168 ± 8.6 cm. Among the concomitant diseases leading to dialysis, hypertension, with the frequency of 43%, was the most common. The mean score of dialysis quality was 1.5 ± 0.6, the duration of dialysis was 6.2 ± 0.4 years, the length of underlying diseases leading to dialysis was 8.4 ± 1.3 years, the time of each dialysis session was 3.6 ± 0.24 hours, and the number of sessions required for dialysis per week was 3.2 ± 0.29. The highest mean scores of QOL were 44.6 ± 6.2 in the men, 42.7 ± 5.8 in the married, and 41.2 ± 6.9 in those with high levels of education and those with an income level of above five million tomans. Among the individual and clinical characteristics, the mean score of QOL was significantly correlated with age (P = 0.03), level of education (P = 0.03), and time of each dialysis session (P = 0.005) (Table 1). The mean score of QOL was 40 in the physical health dimension and 43 in the mental health dimension. The highest and the lowest mean scores of QOL were observed for the physical function (52.8 ± 18.3) and physical pain (32.8 ± 16.6), respectively (Table 2). The mean score of QOL on the physical function scale had a significant relationship with age (P = 0.02) and marital status (P = 0.06), and the highest mean score on the physical function scale was in the age group of < 25 years (69.8 ± 26.3) and the single participants (72.2 ± 19.6). Furthermore, among the QOL scales, the general health scale had a significant relationship with the duration of dialysis sessions (P = 0.05); the highest mean score on this scale was observed for the three-hour sessions (41.2 ± 6.9). Among the QOL dimensions, there was a significant relationship between the mean score of physical health with marital status (P = 0.03), age (P = 0.04), and duration of each dialysis session (P = 0.02); however, other individual and clinical variables had no significant relationship with each other. Moreover, a significant relationship was observed between the mean score of the mental health dimension and marital status (P = 0.01) (Table 3).
| Variables | No. (%) | Mean ± Standard Deviation | P-Value | Correlation Coefficient (R) |
|---|---|---|---|---|
| Gender | 0.1 | 0.12 | ||
| Male | 128 (64) | 44.6 ± 6.2 | ||
| Female | 72 (36) | 39.7 ± 5.4 | ||
| Level of education | 0.03 | 0.02 | ||
| Elementary | 69 (34.5) | 37.3 ± 5.4 | ||
| diploma | 74 (37) | 39.2 ± 6.1 | ||
| University graduates | 57 (28.5) | 41.2 ± 6.9 | ||
| Job | 0.3 | 0.1 | ||
| Employee | 39 (19.5) | 44.4 ± 9.7 | ||
| Freelance work | 102 (51) | 42.9 ± 7.2 | ||
| workless | 59 (29.5) | 40.1 ± 5.8 | ||
| Marital status | 0.6 | 0.02 | ||
| Married | 147 (73.5) | 42.7 ± 5.8 | ||
| Single | 36 (18) | 41.4 ± 6.1 | ||
| Other | 17 (8.5) | 38.6 ± 2.8 | ||
| Income (million tomans) | 0.3 | 0.3 | ||
| ≤ 3 | 27 (13.5) | 40.6 ± 5.8 | ||
| 3 - 5 | 134 (67) | 41.2 ± 0.5 | ||
| 5 ≤ | 39 (19.5) | 41.8 ± 6.3 | ||
| Duration of each dialysis session (hr) | 0.005 | 0.2 | ||
| ≤ 3 | 76 (38) | 48.8 ± 7.2 | ||
| 3 < | 124 (62) | 39 ± 6.7 | ||
| Age | 0.03 | 0.3 | ||
| 25 < | 27 (13.5) | 51.6 ± 5.3 | ||
| 25 - 44 | 52 (26) | 44.2 ± 6.9 | ||
| 45 - 64 | 74 (37) | 43.1 ± 8.7 | ||
| 65 ≤ | 47 (23.5) | 38.1 ± 6.1 |
Correlation, Mean, and Standard Deviation of Quality of Life Score Regarding Personal Information and Clinical Factors
| Domains and Scales | Mean ± Standard Deviation |
|---|---|
| Physical function | 52.8 ± 18.3 |
| Physical pain | 32.8 ± 16.6 |
| general health | 38.9 ± 10.6 |
| Physical limitations | 45.7 ± 36.8 |
| Mental health | 41.3 ± 15.4 |
| Social Performance | 43.2 ± 12.3 |
| Energy and vitality | 50.6 ± 21.7 |
| Mental problems | 41.3 ± 35.4 |
| Physical health dimension | 40.7 ± 9.9 |
| Mental health dimension | 43.4 ± 10.7 |
| Overall quality of life | 42.6 ± 7.6 |
Mean and Standard Deviation of QOL Score, Its Domains, and Scales
| Variables | Physical Health Dimension | Mental Health Dimension | ||
|---|---|---|---|---|
| Mean ± Standard Deviation | P-Value | Mean ± Standard Deviation | P-Value | |
| Marital status | 0.03 | 0.01 | ||
| Married | 49.8 ± 12.3 | 47.2 ± 8.3 | ||
| Single | 43.5 ± 12.5 | 44.9 ± 12.6 | ||
| Other | 39.3 ± 16.8 | 40.5 ± 8.7 | ||
| Duration of each dialysis session (hr) | 0.02 | 0.1 | ||
| ≤ 3 | 45.7 ± 12.6 | 46.3 ± 14.6 | ||
| 3 < | 37.3 ± 7.9 | 40.6 ± 8.5 | ||
| Age | 0.04 | 0.3 | ||
| 25 < | 55.3 ± 9.4 | 44.3 ± 4.2 | ||
Mean and Standard Deviation of Physical and Psychological Dimensions of Quality of Life Regarding Personal Profile and Clinical Information
5. Discussion
In the present study, most of the patients undergoing hemodialysis, including the married, had a diploma, a freelance job, and an income range of 3 - 5 million Tomans. Hypertension was the most common concomitant disease leading to CRF. In the hemodialysis patients, QOL was moderate, and the mean score was higher in the psychological dimension than in the physical dimension. This finding was in line with the findings reported by Ashrafi (21). The low QOL, especially in the physical dimension, can be explained by the fact that the occurrence of CRF and treatment methods such as hemodialysis cause changes in individuals’ lifestyle and health status.
Female patients had lower QOL scores than male patients, which can be attributed to seems to be due to more negative perceptions of the disease and the higher prevalence of depression in women than men (22, 23). Nevertheless, there was no significant relationship between QOL and gender, which was consistent with Abbaszadeh et al.’s study (24).
There was a significant relationship between age and mean score of QOL (P = 0.03); hence, the QOL score decreased with increasing age. The relationship between age and the mean score of QOL is quite complicated, which may be due to the complex nature of QOL. Some studies have reported that age has a strong inverse relationship with the average score of the physical dimension of QOL; thus, the body's physical function decreases with age (25). However, older people’s QOL varies depending on their expectations and beliefs and can sometimes be even higher than that of younger individuals (26). In the study by Muqarb et al., no relationship was observed between age and the mean score of QOL (27). In Rimaz et al.’s study, however, the women’s QOL increased with age (28).
There was a significant relationship between the level of education and the mean score of QOL (P = 0.03); hence, the QOL score raised with increasing patients' level of education. This finding was consistent with Sharifnia’s and Rimaz et al.’s (18, 28) studies. In contrast, Namadi Vosoughi and Movahdpoor reported no relationship between this variables in Ardabil. This inconsistency might have been caused by their low sample size (25). By increasing the level of education, patients' awareness of chronic diseases and their ability to cope with their complications increase; hence, their QOL improves as well (29).
Although staff and patients with higher incomes had higher mean scores of QOL than other patients, no significant relationship was observed. Studies have indicated that patients' QOL improve as income increases. This is because patients can meet their medical needs (30).
The duration of dialysis sessions had an inverse and significant relationship with the QOL score (P = 0.005); hence, the patients' QOL scores decreased with increasing the time of dialysis, . This finding was consistent with Okpechi’s and Anees et al.’s (22, 31) studies. This finding shows the significance of interventions to reduce the duration of dialysis to promote QOL.
The mean score of the physical QOL dimension was significantly correlated with age (P = 0.04), marital status (P = 0.03), and duration of each dialysis session (P = 0.02); however, Sathvik et al. found no significant difference in this regard (29). Studies have shown that the presence of a spouse as a supporter can be effective in reducing stress, adapting the treatment regimen, reducing disability, and improving the mental condition of hemodialysis patients (32).
5.1. Conclusions
Many studies have indicated a strong relationship between the low scores of QOL in dialysis patients with increased mortality. Given that changes in various dimensions of QOL are influenced by individual, social and economic factors, evaluating these patients’ QOL and identifying their demographic characteristics provide useful information to health managers. Moreover, since there is an inverse correlation between the QOL scores with age and duration of dialysis sessions, indicating the effect of age on the physical dimension, promoting the quality of services such as physical support is necessary to reinforce policies and programs for dialysis patients across the country.
