
1. Background
After surgery, the procedure for finishing the fascia should be quick, easy, and persistent but comfortable for the patient with minimum complications at the surgery site, such as infection and hernia or formidable fascia dehiscence. Non-absorbable threads, such as nylon and polypropylene stitch, are commonly used in fascia repair. However, the polydioxanone (PDS) thread has attracted lots of interest due to its favorable macrophage response (1).
Wound complications might be annoying or even lethal. Abdominal incision opening has a frequency of up to 4%, and it is a dreaded initial problem after a belly operation with sequelae similar to evisceration, lengthy hospitalization, and great death rates (2). Furthermore, the incisional hernia is a communal impediment after midline cuts, with a 5-30% occurrence that may affect aching, abridged quality of life, and great healthcare expenses (3). Numerous suture ingredients and methods for closing the slits have been scrutinized; however, there is still a requisite for closure methods to prevent incisional hernia.
The existing approval is to practice the slight bites method (i.e., 5 mm flesh bites and 5 mm amid two sutures) with sluggishly absorbable stitch ingredients for closing the fascia (4). However, based on the biomechanical issues, the significance of the bite technique remains unidentified (5). A stitch might get through flesh owing to confined force or strain, which might scratch through flesh instantly, ensuing in a ruptured abdomen or an incisional hernia after a while from troubled healing by infection and/or flesh necrosis (6).
Nevertheless, this thread is not widely available in Iran; thus, Vicryl was employed for almost all patients to avoid the disadvantages of non-absorbable sutures. Reports of these patients are presented in this study. This descriptive cross-sectional study was conducted at Imam Reza and Imam Khomeini Medical Centers in Ardabil from January 2018 to January 2020. Using the whole sampling method, we included 642 patients in this study.
2. Methods
The fascia of all patients in the Urology Department was treated with the Vicryl suture with the size of 0 or 1 in a double layer and a continuous manner. These patients underwent varicocele surgery, inguinal hernia in children and adult patients, open prostate (retropubic or suprapubic) surgery, radical prostatectomy surgery, radical kidney transplant surgery (radical cystectomy), bladder stone surgery (cystolithotomy), partial cystectomy, ureterolithotomy, ureterocystostomy, radical nephrectomy, partial nephrectomy, nephrolithotomy, and adrenalectomy. During this time, the Vicryl suture was used in children, adults, and patients with or without a history of surgery. The sutures were made at a 1-cm distance from the adjacent ones and the edge of the fascia. The fascia was repaired in two layers, and each muscle layer was separately sutured. In larger incisions, the suturing began separately from the two ends of the wound. The nodes in the center were made with two sutures, and the sutures were returned to the top of the wound and tied with the end (at least four nodes). In smaller wounds, such as varicocele or inguinal hernia, the suture began from one end of the wound, returned backward to start the second layer of the suture, and then was tied. The subcutaneous tissue was usually treated with chrome, and the skin was amended by nylon. Prophylactic antibiotics (cefazolin and clindamycin in case of allergy) were used 30 minutes before the surgery. One surgeon performed all surgeries. Patients were followed up for six months to two years for infection, dehiscence, hernia, and pain at the wound site. Overall, 642 patients were assessed in these two years (2018 - 2020). The fascia handling was at the inguinal, midline, Gibson, and flank regions. The fascia treatment was made for each patient by Vicryl continuously in two layers. Due to the lack of inclusion and exclusion criteria, all patients were included in the study.
3. Results
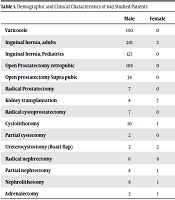
The present study was conducted on 636 urologic patients, including 100 varicocele patients, 203 adults with inguinal hernia, 123 pediatrics with inguinal hernia, 108 retropubic prostatectomy patients, 34 suprapubic (transvesical) prostatectomy patients, seven radical prostatectomy patients, 11 kidney transplantation patients, seven radical cystoprostatectomy patients, 11 cystolithotomy patients, two partial cystectomy patients, four ureterocystostomy patients (Boari flap), 15 radical nephrectomy patients, five partial nephrectomy patients, nine nephrolithotomy patients, and three adrenalectomy patients. Of 203 adults with inguinal hernia repairs, just one case had a surgical site infection. He was a 66-year-old man with diabetes mellitus and severe obesity. His infection was relieved after a two-week antibiotic therapy (co-amoxiclav and ciprofloxacin).
Of 108 patients who underwent retropubic prostatectomy, just a case showed an incisional hernia without additional treatment. He also suffered from diabetes mellitus. He used a specific garment to support an incisional hernia. One of the 34 patients with suprapubic prostatectomy got a surgical site infection treated with a two-week intravenous antibiotic therapy (meropenem and gentamicin). He had no specific medical history except for a two-month carrying Foley for urinary drainage because of recurrent urinary retention. Escherichia coli caused the infection.
One patient with radical nephrectomy due to renal cell carcinoma showed a hernia at the flank incisional site. The patient was a 59-year-old woman with a body mass index (BMI) of 34.5. She got incisional hernia repair surgery with mesh placement (Table 1). The data showed that incisional hernia and infection were more prevalent in obese and diabetic patients. We had no incisional complications in radical cystectomy or even kidney transplantation patients that had complicated and time-consuming surgeries. Overall, the surgical site complication rate (including incisional hernia and surgical site infection) was 0.9%, which could be negligible.
| Male | Female | Age | BMI | DM | Complications | |
|---|---|---|---|---|---|---|
| Varicocele | 100 | 0 | 13 -31 | 18 - 34 | - | - |
| Inguinal hernia, adults | 201 | 2 | 21 -75 | 20 - 32 | 144 | One surgical site infection |
| Inguinal hernia, Pediatrics | 123 | 0 | 1 - 12 | - | ||
| Open Prostatectomy retropubic | 108 | 0 | 59 - 89 | 26.7 - 33 | 99 | One incisional hernia |
| Open prostatectomy Supra pubic | 34 | 0 | 66 - 74 | 24.6 - 35 | 29 | One surgical site infection |
| Radical Prostatectomy | 7 | 0 | 65 - 81 | 22.1 - 26.5 | 2 | - |
| Kidney transplantation | 4 | 7 | 24 - 65 | 23 - 30.1 | 0 | - |
| Radical cystoprostatectomy | 7 | 0 | 47 - 76 | 22 - 27 | 1 | - |
| Cystolithotomy | 10 | 1 | 42 - 78 | 24.4 - 36 | 9 | - |
| Partial cystectomy | 2 | 0 | 78 -85 | 28.7 - 30.6 | - | - |
| Ureterocystostomy (Boari flap) | 2 | 2 | 44 - 56 | 22.2 - 25.7 | - | - |
| Radical nephrectomy | 6 | 9 | 39 - 78 | 24.7 - 34.5 | - | One incisional hernia |
| Partial nephrectomy | 4 | 1 | 67 - 70 | 27.6 - 28.2 | 2 | - |
| Nephrolithotomy | 8 | 1 | 26 - 54 | 21.9 - 27 | 3 | - |
| Adrenalectomy | 2 | 1 | 65 - 69 | 24 - 26.1 | 2 | - |
Demographic and Clinical Characteristics of 642 Studied Patients
4. Discussion
No similar research has addressed fascia suturing in the field of urology. For closing infection-suspicious fascia, it is better to apply the sutures individually. However, the preferred suture material has not been confirmed (7). Nevertheless, comparing PDS with Prolene sutures showed the superiority of PDS, primarily when sutures are performed with 5-mm intervals (4). Vicryl suture maintains its strength in kidney parenchyma; thus, it is more acceptable than other sutures (8). Vicryl suture is a synthetic, biocompatible, and regenerative tool that minimizes tissue reaction complications of surgical wounds. Surgical wounds are divided into early and late forms. Early complications include infection, dehiscence, or sinus formation at the site of the wound, while herniated surgical site and chronic pain are among the late complications. The kind of stitch may influence the incisional outcome. Applying Vicryl sutures in midline fascia repair instead of non-absorbable ones does not increase wound complications (9, 10).
Many surgeons still apply nylon sutures for fascia repair and are afraid of absorbent types. Although studies assessing suture material on incision complications are widespread in general surgical procedures, a limited number of studies have addressed them in urology operations. Previous research has publicized more contamination rates in the non-absorbable (Prolene and PDS) sutures (11). Non-absorbable sutures also increase sinus formation in the healing suture line of fascia in the company of lasting discomfort. Operational time is so critical in the contamination of the wound. However, the rate of wound and hernia infections in the surgical area was negligible in our patients, potentially due to a cleaner urologic surgical environment and a shorter duration of surgery. In urologic surgeries, the intestine is only opened in the case of radical cystectomy. Even in such cases, no wound infection or hernia was observed in our patients.
Regarding renal transplantation, where the patient's immune system was compromised, no wound infection, wound dehiscence, or hernia was detected at the surgical site. There have been more reports of the breach of the wound and pseudo-infection with the absorbable (Vicryl) suture (12). In this study, all surgeries were elective and non-emergent, performed by the same surgeon, which can explain the low rate of surgical site complications. The rate of hernia and wound breach is lower in monolayer mass closure compared with multi-layered closure, despite multi-layered suturing of the muscles and fascia. However, continuous mass closure of midline fascia with Vicryl led to satisfactory results. Discomfort in the incisional region was minor in absorbable stitches like Vicryl, which confirms our study (13).
There is still much controversy about the type (absorbable or non-absorbable) and pattern (continuous or interrupted) of the suture in incision complications (14, 15). Notably, the appropriate suture should be selected depending on the procedure. Some prefer the continuous form as it spreads pressure throughout the wound and decreases tissue ischemia. However, much evidence in the urologic field regarding fascia repair is granted from general surgery (16). On the contrary, interrupted suturing can lead to wound infection and incision hernia by creating ischemia and necrosis due to multiple nodes and varying degrees of node tension. Finally, the type of knot (forwarder or surgeon knot) might affect suture outcomes (17). The PDS suture is superior, but it was not employed in our center due to its high cost and scarcity.
4.1. Conclusions
The fascia repair could be treated with Vicryl suture in a continuous form in all urologic surgeries, with a very low rate of wound infection and hernia at the operation site, sinus formation, and long-term surgical site discomfort. However, we suggest more research to confirm the Vicryl suture safety in urologic fascia repairs.
4.2. Limitations
Performing this pioneering study was very difficult regarding the popularity of nylon suturing in the fascia.
