




1. Background
Erectile dysfunction (ED) is a common sexual dysfunction in men and is defined as the inability to attain or maintain an adequate penile erection during sexual intercourse, impeding the achievement of a satisfactory sexual activity (1). Disruption of any component of the erection response, such as organic, relational, and psychological factors, can cause ED (2). A wide range of external signals, including visual, auditory, and olfactory signals, as well as penile local stimuli, can disrupt the erection response through a complicated physiological cascade involving neurologic, vascular, and humoral processes (3). The erection process is triggered by the activation of the parasympathetic system, which leads to decreased levels of intracellular calcium, the relaxation of cavernosal smooth muscles, and increased blood flow (4). According to an epidemiological study, the prevalence of ED in all age groups in southern Europe and English-speaking countries was reported to be 12.9% and 20.6%, respectively (5). An updated retrospective cross-sectional study assessed the prevalence of ED in eight countries that had a great burden of the disease, reporting an overall prevalence of ED varying from 37% in Brazil to 49% in Italy (5). Erectile dysfunction has detrimental impacts on patients’ quality of life and self-esteem. Moreover, it can cause deleterious psychological symptoms such as depression and anxiety in patients, and these effects can also affect their sexual partners (1, 2). As ED results from a complicated interaction between psychological and physiological processes, American Urological Association (AUA) guidelines recommend mental health counseling as an adjunctive treatment for affected individuals (6). Erectile dysfunction has been reported to be associated with endothelial dysfunction, such as impaired nitric oxide/cyclic guanosine 3′5′-monophosphate (NO-cGMP) signaling pathway. Thus, ED can be an early manifestation and predictor of generalized endothelial dysfunction and related abnormalities, as well as other forms of cardiovascular diseases (7). The risk factors of ED include age, depression, obesity, cardiovascular disease, hypertension, diabetes mellitus, and spinal cord injury, as well as psychological factors (7, 8).
Therapeutic options for ED vary from non-invasive to invasive therapy and include lifestyle modification, oral drugs, intracavernosal injections (ICIs), vacuum-assisted erectile devices (VED), and penile prostheses, as well as novel treatments, such as stem cell therapy, shockwave therapy, and the use of platelet-rich plasma (9). Common oral medications are sildenafil, tadalafil, vardenafil, and avanafil, which act as an inhibitor of phosphodiesterase type 5 (PDE5) (9). Oral medications are the first line of therapy in patients with refractory to lifestyle changes; approximately 60 - 65% of men diagnosed with ED, and those with other comorbidities such as hypertension, diabetes mellitus, and spinal cord injury, show successful treatment to complete intercourse of PDE5 inhibitors (10-13).
We found no well-designed study on the effect of spinal anesthesia on erectile function in patients undergoing surgeries, particularly urologic endoscopic surgeries and other types of procedures that need spinal anesthesia. In addition to the association between spinal anesthesia and erectile function, studies have shown that spinal anesthesia leads to changes in penile length during and after surgery. A growing body of evidence has demonstrated that spinal anesthesia can lead to priapism, which is defined as the prolonged erection of the penis without any sexual arousal/desire. Priapism is a relatively rare phenomenon that may occur as a result of an imbalance between the sympathetic and parasympathetic nervous systems. This phenomenon can bring significant troubles, such as excessive bleeding, for surgeons and other medical teams during surgeries (14, 15).
2. Objectives
In this study, we aimed to divulge the association of spinal anesthesia with erectile function and penile length during and after surgery. Moreover, selecting an appropriate type of anesthesia for patients with erectile dysfunction to avoid alterations in penile length can facilitate the decision-making process about the preferable anesthetic agent for these patients during urological surgeries.
3. Methods
3.1. Study Design
Details of this part of the study have been blinded due to the journal’s request.
3.2. Study Population
Patients aged between 18 and 60 years old were enrolled in this study. Inclusion criteria were endoscopic surgeries that do not affect patients’ sexual activity, including trans ureteral lithotripsy (TUL), cystoscopy, and ureteroscopy. Patients with a history of trauma to the urogenital tract, prostate surgery, pelvic radiation, and other surgeries that affect sexual activity, such as transurethral resection of the prostate (TURP), were excluded from this study. Moreover, patients with sensitivity to certain anesthetic agents and those who were unwilling to receive spinal anesthesia were excluded from the study.
The sample size was estimated based on the power calculation, showing that at least 40 patients per group were required to achieve α=0.05 and to detect a 20% difference between the two study groups with a power (β) equal to 80%. As we found no similar study, the difference was predicted to be two units of the questionnaire’s score.
3.3. Randomization, Blinding, and Intervention
The participants were randomly assigned into two groups of 40 subjects using a computer-generated table of random numbers. We used sealed envelopes to achieve allocation concealment. In this study, all the patients were blinded to the study procedure and treatments. The second author of the study delivered anesthetic agents to a nurse anesthetist in a blinded manner. In the spinal anesthesia (SA) group, following skin cleansing in a seated position, a 25-gauge Quincke needle was entered into the intrathecal space through the L3-4 interspace. Then 12.5 - 15 mg of hyperbaric bupivacaine 0.5% was administered after the free flow of cerebrospinal fluid was observed. In the next step, patients in the SA group received propofol for sedation and muscle relaxation (25 µg/kg/min) and narcotic agents (fentanyl, 1 µg/kg IV stat) and midazolam (0.02 mg/kg) for sedative effects. Patients in the general anesthesia (GA) group received propofol (1 - 2 mg/kg), fentanyl (1 µg/kg IV stat), and midazolam (0.02 mg/kg) to obtain narcotic effects and muscle relaxation. All patients received 0.15 mg/kg cisatracurium, and the endotracheal tube was then administered to deliver the inhalation agent (sevoflurane 2 - 3%) and achieve mechanical ventilation. Penile length was measured in centimeters from the penopubic junction to the urethral meatus. A straight-edge tape was administered to measure the distance between the penopubic junction and the urethral meatus along the dorsum of the penis in both flaccid and stretched states before, immediately after, and two weeks after the intervention.
3.4. Outcome Measurement
The primary objective of this study was to assess changes in penile length following spinal anesthesia in comparison with general anesthesia. Our secondary goal was to evaluate sexual function based on the international index of erectile function (IIEF)-5 score in the two groups of patients.
3.5. Statistical Analysis
We analyzed all patients’ data based on an intention-to-treat principle. We used SPSS software (version 23) to analyze the data. Quantitative variables were reported as mean ± standard deviation (SD), and repeated measure ANOVA was used to evaluate changes in penile length in both stretched and flaccid states in each group. Moreover, the independent sample t-test was utilized to compare the IIEF-5 score between the two groups at predetermined time intervals. In all statistical tests, P value < 0.05 was considered statistically significant.
4. Results
4.1. Subjects’ Clinical and Baseline Characteristics
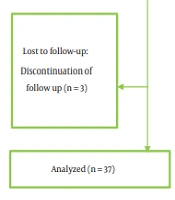
The CONSORT flowchart is shown in Figure 1. Overall, 73 men (37 in the SA group and 36 in the GA group) referring to the Shohada-e-Tajrish Hospital for endoscopic surgeries were included in this study. Differences in the participants’ baseline characteristics between the two groups were not statistically significant (Table 1). Mean ages in the SA and GA groups were 39.03 ± 15.81 and 38.95 ± 14.28 years, respectively. Erectile function was assessed based on the IIEF-5 score. Based on this questionnaire, the cases of ED were categorized as follows: Severe (scores 5 - 7), moderate (scores 8 - 11), mild to moderate (scores 12 - 16), mild (scores 17 - 21), and no ED (scores 22 - 25). According to the score obtained from the IIEF-5 questionnaire, patients in both the SA and control groups were placed in the mild ED category. Mean IIEF-5 scores in the SA and control groups were 21.13 ± 2.46 and 23.68 ± 1.33, respectively, showing no significant difference between the two groups (P value < 0.1). Table 2 shows the number of patients with comorbidities and a history of taking certain medications.

The CONSORT flowchart illustrating the process of patient screening in this study.
| Type of Anesthesia | N | Spinal Anesthesia Group | General Anesthesia Group | P Value |
|---|---|---|---|---|
| Age (y) | 40 | 39.03 ± 15.81 | 38.95 ± 14.28 | 0.98 |
| Duration of surgery (h) | 40 | 1.45 ± 1.31 | 1.25 ± 0.71 | 0.39 |
| Mean IIEF score before surgery | 40 | 21.13 ± 2.46 | 19.98 ± 2.71 | 0.10 |
| BMI (kg/m2) | 40 | 23.4 ± 1.5 | 23.68 ± 1.33 | 0.38 |
Abbreviations: IIEF, international index of erectile function; BMI, body mass index.
| Comorbidities/Medications | Type of Anesthesia | Total | |
|---|---|---|---|
| Spinal | General | ||
| History of trauma | 1 | 1 | 2 |
| History of PF | 0 | 0 | 0 |
| History of urinary tract trauma | 1 | 1 | 2 |
| History of trauma to the penis and genital system | 1 | 0 | 1 |
| Spinal cord surgery | 0 | 0 | 0 |
| Spinal cord disease | 0 | 1 | 1 |
| Peyronie’s disease | 0 | 0 | 0 |
| MS | 0 | 0 | 0 |
| Parkinson’s disease | 0 | 0 | 0 |
| DM | 1 | 1 | 2 |
| HID | 0 | 1 | 1 |
| CAD | 0 | 0 | 0 |
| HLP | 1 | 1 | 2 |
| Thyroid disease | 0 | 0 | 0 |
| Opium | 0 | 2 | 2 |
| Alcohol consumption | 0 | 1 | 1 |
| Anabolic steroids | 0 | 0 | 0 |
| Beta-blockers | 0 | 0 | 0 |
| Antihypertensive medications | 0 | 2 | 2 |
| Hormone therapy | 1 | 1 | 2 |
| Radiotherapy | 0 | 0 | 0 |
| Psychology | 0 | 0 | 0 |
| Depression | 0 | 1 | 1 |
| Psychiatric medications | 0 | 0 | 0 |
| Other comorbidities | 0 | 0 | 0 |
| Sedation | 0 | 0 | 0 |
Abbreviations: MS, multiple sclerosis; DM, diabetes mellitus; HID, heart ischemic disease; CAD, coronary artery disease; HLP, hypolipoproteinemia.
4.2. Flaccid Penile Length During and Two Weeks After the Intervention
At the baseline, the means of penile length in the flaccid state before the intervention in the SA and control groups were 9.89 ±1.26 and 10.03 ± 2.09 cm, respectively, showing no significant difference according to Student’s t-test (P-value < 0.3). Table 3 shows the mean penile length in the flaccid state in both study groups during and two weeks after surgery.
| Type of Anesthesia | Spinal Group | General Group | P Value |
|---|---|---|---|
| Mean penile length during surgery (cm) | 9.21 ± 1.73 | 10.26 ± 2.7 | 0.33 |
| Mean penile length two weeks after surgery (cm) | 9.68 ± 1.8 | 10.36 ± 2.5 | 0.33 |
We conducted a series of repeated-measure ANOVA designating the baseline penile length as the covariate to check changes in the flaccid penile length over time. Repeated-measure ANOVA demonstrated that compared to the baseline, there was no significant difference in penile length during and two weeks after the intervention in the SA and control groups (P value = 0.33). The difference in changes in flaccid penile length was not statistically significant between the two groups during the surgery. Penile length in the flaccid state increased two weeks after the intervention in both groups; however, the difference was not significant between the two groups (P value = 0.33, Table 3).
4.3. Stretched Penile Length During and Two Weeks After the Intervention
Before the intervention, the means of penile length in the erect state were 13.03 ± 1.22 and 14.63 ± 2.54 cm in the intervention and control groups, respectively. Based on the student’s t-test, there was no significant difference in the baseline erect penile length between the two groups (P value < 0.45). Table 4 shows the means of penile length in the erect state in both the SA and control groups during and two weeks after the intervention.
| Type of Anesthesia | Spinal | General | P Value |
|---|---|---|---|
| Mean penile length during surgery | 14.38 ± 1.29 | 13.25 ± 2.42 | 0.35 |
| Mean penile length two weeks after surgery | 14.78 ± 1.32 | 13.36 ± 2.41 | 0.35 |
Compared to the baseline, repeated-measure ANOVA showed a non-significant difference in the erect penile length during and two weeks after the intervention in both the intervention and control groups (P = 0.4). Two weeks after the intervention, changes in stretched penile length were not significant in the two study groups (P = 0.25); however, erect penile length in the intervention group showed more changes than the control group, which was not statistically significant between the two groups (P = 0.35, Table 4).
4.4. IIEF Changes in the Two Study Groups
Before the intervention, the mean score of the IIEF-5 questionnaire was 21.13 ± 2.46 in the SA group and 19.98 ± 2.71 in the control group, indicating no significant difference according to student's t-test (P value < 0.1). Table 5 shows the mean score of the IIEF-5 questionnaire before and one month after the intervention in both study groups. The repeated-measure test revealed that the mean IIEF-5 score was significantly lower in the SA group than in the control group at one month post-intervention (P < 0.001, Table 5).
| Type of Anesthesia | Spinal | General | P Value (Time) |
|---|---|---|---|
| IIEF score before surgery | 21.13 ± 2.46 | 19.98 ± 2.71 | < 0.05 |
| IIEF score one month after surgery | 18.38 ± 2.28 | 20.55 ± 2.08 | < 0.05 |
Abbreviation: IIEF, international index of erectile function.
One month after the intervention, the SA group showed a statistically significant decrease in the mean IIEF-5 score compared to the control group (Table 5); however, regarding IIEF severity, participants in both groups were identified to have mild ED.
After three months of the surgery, the IIEF-5 score was determined in both groups again, revealing no significant difference between the two groups. No priapism or major complications due to anesthetics were reported by the participants.
4.5. Loss to Follow-up
Three patients in the SA group and four patients in the GA group were lost to follow-up due to either contracting the COVID-19 infection, not having regular sexual activity, or going on vacations.
5. Discussion
It has been reported that following SA, penile length is increased compared to before anesthesia. In this regard, we found no well-designed studies to address this issue, and available studies either lack control groups or are case reports. To the best of our knowledge, this is the first well-designed blinded controlled trial assessing the effect of SA on penile length and ED. In this study, we examined the effect of SA on penile length in the flaccid and stretched states in comparison with GA. According to our results, the mean penile length did not significantly change during surgery compared to pre-surgery. However, a study conducted by Fyneface-ogan et al. reported that there was a significant change in penile length following SA. One possible explanation is that SA impairs the sympathetic and parasympathetic innervation of the penis, leading to penile enlargement or even penile erection (14).
Another important issue that should be considered following spinal or general anesthesia is unplanned penile erection, which can lead to excessive bleeding and urethral trauma. Intraoperative penile erection (priapism) is a rare event, and its exact mechanism is unclear (16). Priapism is defined as the persistent and painful erection unrelated to sexual desire or sexual excitement (17). A possible explanation may be the activation of the sacral segments of parasympathetic pathways that seem to remain unblocked after anesthesia, resulting in the relaxation of corporal arterioles and subsequent corpora engorgement, leading to erection (18, 19). As another possible mechanism, anesthetic agents can inhibit the brain’s cortical centers involved in the depression of penile erection, promoting an erectile response after tactile stimulation (15). An intraoperative penile erection should be managed carefully in order to reduce its deleterious postoperative effects, including thrombosis and fibrosis. If priapism sustains for more than four hours, it can lead to edema, enhanced risk of abrasion, penile necrosis, and tissue degeneration (15). It is worth mentioning that intraoperative penile erection can occur during both spinal and general anesthesia. Nevertheless, priapism was not observed in any of our patients; however, one should be aware of its proper management.
We also examined the effect of SA on the sexual function of our patients. To the best of our knowledge, until today, there is no study investigating the effect of anesthesia on the sexual function of men. According to our results, SA can be associated with transient sexual dysfunction in men undergoing surgery. We evaluated the sexual function of our patients through the IIEF-5 questionnaire. Our results showed that patients in the SA group experienced short-term sexual dysfunction, including the inability to achieve an erection during sexual activity, difficulty with erection maintenance, decreased sexual desire, and decreased confidence and satisfaction with sexual activity. The mean of the IIEF-5 score after one month of the surgery was significantly lower in the SA group compared to the GA group. However, this effect was short-term, so no significant difference was observed between the two groups three months after the surgery. The administration of appropriate anesthetic agents depends on various factors. For instance, SA seems to be an appropriate anesthetic method to reduce blood loss during urological surgeries; however, this method may lead to cardiovascular and respiratory complications. Overall, SA seems to be safer than GA for patients with sexual dysfunction, a notion that should be considered by practitioners when choosing anesthetic agents for patients with sexual dysfunction. Until today, the exact reason for this event remains unclear, but it may be due to neuronal or vascular damage during anesthesia. More studies are needed to confirm our results and the association observed between SA, rather than GA, and sexual dysfunction during the first-month post-intervention.
This was the first study on an Iranian population indicating that there was no difference between SA and GA regarding the occurrence of ED, including changes in penile length, within two weeks post-surgery. Nevertheless, we observed that SA led to transient ED, which was short-term and resolved within three months after surgery.
5.1. Limitations
The major limitation of this study was its small sample size, which could have affected the findings. In the current study, the duration of surgeries was short; therefore, lower doses of anesthetic agents were required. So, different results may be observed in patients undergoing long surgeries requiring higher doses of anesthetic drugs. Another limitation of the present study was the age of the patients enrolled, most of whom were young (younger patients generally experience milder ED compared to older patients). Thus, our results may not be applicable to older patients who can experience severe ED. Finally, the IIEF-5 questionnaire measures erectile function only over the past six months; however, this was the only standardized questionnaire validated for Persian language people.
