





1. Background
Bladder cancers (BC) are classified into two groups according to histological type: Epidermoid type and urothelial carcinomas (1). Due to their magnitude and severity, these cancers constitute a public health problem in Ivory Coast. Bladder cancers occur frequently around the fifth decade of life, occupying the second rank of urological cancers after prostate cancer and representing the leading cause of cancer mortality in urology (2). In Ivory Coast, at least 4 out of 5 urinary cancers are bladder cancers (3).
2. Objectives
Few studies in Ivory Coast have addressed the risk factors associated with mortality from BC. Thus, the general objective was to study the factors of poor prognosis in BC.
3. Methods
3.1. Location, Duration and Period of Study
This was a retrospective cohort study conducted over a 10-year period (from 2013 to 2022) at the Urology Department of the Abidjan-Cocody University Hospital Center (UHC).
3.2. Study Population
Out of 114 files listed, only 74 complete and usable files (64.9%) were retained, while 40 files (35.1%) were excluded from the study due to being incomplete.
3.3. Inclusion Criteria
Included were all cases (74) of bladder cancer confirmed by additional examinations (ultrasound, uroscan, cystoscopy, and anatomopathological examination) and whose follow-up was carried out exclusively in the said department.
3.4. Exclusion Criteria
Forty patients were withdrawn due to incomplete medical records; some were referred outside the country, and others to private centers.
3.5. Collection and Study of Variables
Data collection was conducted by reviewing medical records and operative reports using a standardized survey form. The variables studied included patients' age, occupation, income, health insurance, histological type, reason for consultation, treatment received, postoperative hemorrhage/hemoglobin level, tumor size, consultation time, and mortality rate.
3.6. Ethical Consideration
- The study was conducted in the Urology Department of the Cocody University Hospital, requiring the favorable opinion of the head of the department and the medical and scientific director of the Cocody University Hospital, who is responsible for the establishment's ethics committee.
- Patient consent was not required since this is a retrospective study.
- Nevertheless, the medical data of each patient were transmitted only to the principal investigator or any person authorized by the latter under conditions guaranteeing their confidentiality. The procedures followed were in accordance with the ethical standards of the Declaration of Helsinki (amendment 2008) of the World Medical Association.
4. Results
- The mean age was 56.59 years, with extremes of 28 and 78 years.
- There was a male predominance of 74.32%.
- The majority of patients were workers and farmers.
- The reasons for consultation were dominated by hematuria at 70.8%.
- The mortality rate was 46% (34 deaths). At cystoscopy, 83.3% of cancers had a budding appearance, and 74.1% were large (> 6 centimeters).
- The histology was predominantly of the epidermoid type, accounting for 71.4%.
- Patients with bladder cancer whose postoperative course was complicated by hemorrhage with severe anemia were all deceased.
- The correlation between the mortality rate and hemorrhagic complications was statistically significant (χ2 observed = 67.40 > χ2 critical = 3.84).
5. Discussion
The mean age of the patients was 56.59 years, with age extremes of 28 and 89 years. These results are consistent with the international literature, which indicates that bladder tumors occur mainly in the elderly (3, 4). Burger et al. (5) reported that the incidence of bladder tumors increases significantly after 40 years, with a mean age of diagnosis of 69 years in men and 71 years in women. Similarly, Benchekroun et al. (3) in Morocco reported a mean age of discovery varying between 59 and 62 years. The male predominance observed in this study (74.32%) was also in agreement with global data (6). Siegel et al. (7) reported that bladder cancer is more common in men, with a male-to-female ratio of approximately 3 to 1. This gender disparity could be explained by more frequent exposure of men to major risk factors, such as smoking and urinary schistosomiasis (5). Indeed, Burger et al. (5) highlighted that smoking is a major risk factor for bladder tumors, with a higher prevalence in men in many parts of the world. In addition, urinary schistosomiasis, endemic in some parts of Africa, is a significant risk factor for bladder epidermoid type (Table 1), which was the dominant histological type in our study (71.4%) (8). The annual mortality rate was 46%. This rate has been reported by some Malian authors such as Cissé et al. (1), who found 45% and 37%, respectively, while Sine et al. (9) in Senegal observed an overall cancer death rate of 51.5%, with bladder cancer accounting for 23.6% of these deaths. These figures contrast sharply with those in developed countries. For example, Siegel et al. (7) reported that in the United States, the bladder cancer mortality rate is approximately 4.5 per 100,000 population, which is significantly lower than the rates observed in Africa. This difference may be explained by several factors, including earlier diagnosis, better access to treatment, and a lower prevalence of specific risk factors such as schistosomiasis in developed countries (10).
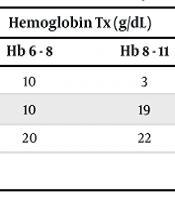
Factors associated with mortality in this study included tumor size (Table 2), severe anemia, and postoperative complications. Patients with tumors larger than 6 cm had a 100% mortality rate, which is consistent with international studies. Shariat et al. (11) showed that tumor size is an independent prognostic factor in bladder cancer, with larger tumors associated with an increased risk of progression and mortality (Table 2). Similarly, severe anemia (Hb < 6 g/dL) was strongly associated with mortality in our study (Table 3), consistent with the results of Ploussard et al. (10), who highlighted that anemia is a poor prognostic marker in urological cancers. Histological type also played a significant role in mortality, with the epidermoid type accounting for 88.2% of deaths. In the series, deaths observed in patients with squamous cell carcinoma bladder tumors accounted for 30 out of 34 cases, or 88.2%, and there was a statistically significant association between cancer type and mortality. This result aligns with the observations of Cissé et al. (1), who reported that 82.14% of deaths were associated with this histological type (Table 1). Squamous cell carcinoma is particularly aggressive and often diagnosed at an advanced stage, which explains its impact on mortality (12). In contrast, in Western countries, urothelial carcinoma is more common and generally associated with a better prognosis (13). Postoperative complications, particularly hemorrhage, were also a major risk factor for mortality in this study (Table 3). All patients with postoperative hemorrhage died. This finding highlights the importance of optimal perioperative management to reduce complications and improve survival.
Finally, delay in consultation and lack of access to care were identified as contributing factors to the high mortality observed in this study. Salah et al. (14) highlighted that in many African countries, patients often consult at an advanced stage of the disease, which limits therapeutic options and worsens the prognosis. Furthermore, Houede et al. (15) noted that socioeconomic barriers, such as poverty and lack of health insurance, play a crucial role in access to care and clinical outcomes. In some West African countries, bladder cancers are often discovered late, and in certain regions, the epidermoid types are the most numerous and very aggressive, often favored by bilharzia. Effective and less expensive treatment must be based on prevention. This prevention must be undertaken by public authorities by effectively treating the primary infection of bilharzia in childhood. Prevention is done in two stages: Collective prevention through the use of anti-bilharzia measures and individual prevention through awareness-raising for individual protection, consisting of breaking the chain of bilharzia contamination by cleaning up ponds in marshy regions of stagnant water to destroy the larval breeding sites of the intermediate hosts (bulins) of bilharzia.
5.1. Conclusions
The mortality rate of bladder cancers is high in the Urology Department of the CHU of Cocody. Hematuria is the main symptom of admission. The epidermoid type, large size of the bladder cancer, and post-surgical hemorrhagic complications are risk factors for mortality of bladder cancers.
