1. Background
Infectious diseases in the neonatal population and their treatment is a common problem in pediatrics (1). Since combination of ampicillin and aminoglycosides as an approved treatment of choice has been used in infections, yet they all have many important side effects and studies have not evaluated these effects (2, 3). Due to high concentration of aminoglycosides in the renal cortex, this drug may have side effects on the kidneys, such as nephrotoxic effect, indicated by an increase of serum creatinine, from its baseline, in range of 0.5 or more than 0.5 milligrams per deciliter. In contrary to the therapeutic effects of aminoglycoside, this toxicity is not dose-dependent (4). Therefore, high or low concentration of aminoglycosides in the cortex of the kidney induces nephrotoxic effects as a common and important side effect (5). Also, increasing duration of treatment with aminoglycosides increases the risk of nephrotoxic effect, so that more than 14 days of treatment increases the risk of nephrotoxic effect to 50% (6, 7). Aminoglycosides induce damage of proximal convoluted tubule, and rarely induce dysfunction of glomeruli. Furthermore, acute tubular necrosis and reduced GFR and anuria can occur at the end, as a life threatening complication and in most cases, the induced nephrotoxic effect by these drugs is irreversible (8). Based on this context, this research found infectious diseases in the neonatal population and its treatment as a common problem. Therefore, the aim of this study was to evaluate the nephrotoxic effects of gentamicin and amikacin in the neonatal population to make better use of medications for infection, with lower nephrotoxic effects.
2. Methods
2.1. Study Settings
This was a double blind clinical trial study, which was hospital-based, conducted in the pediatric clinic of Amir-Kabir and Taleghani hospital of Arak city.
2.2. Study Population
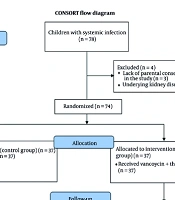
In total, 80 children with complete gestational age, different source of infection, and indication for treatment with aminoglycosides, were evaluated in this study. Based on synchronization the cases were divided to 2 groups. During the study, parents of patients, who wished to discontinue their participation or were not available to complete the study, were assigned by patients with similar clinical and demographic factors.
2.3. Measurements
After selection of children, basic information, including age (day) and gender (male or female) was recorded in the question list and first serum and urine samples were taken from the patients. Children were divided to 2 groups and treated during 7 days by ampicillin or gentamicin; 40 children by ampicillin and amikacin and 40 children by ampicillin and gentamicin. Antibiotics were injected intravenously by micro infusion set and within a 30-minute period. Ampicillin was used for Listeria and group B of Streptococcus, and aminoglycosides were used for enteric gram negatives. Registeration of laboratory variables was done by secondary serum and urine samples. Studied variables included bicarbonate, BUN, creatinine, sodium, potassium, calcium, U/A, and GFR, and nephrotoxic effect was defined as an increase of serum creatinine, from its baseline, in the range of 0.5 or more than 0.5 milligrams per deciliter.
2.4. Antibiotics Doses
Antibiotic doses of the 2 groups were used based on gestational age and weight, as mentioned in Table 1.
Table 1.
Doses of Administered Antibiotics
| Antibioticsa | Postnatal Age | |||
|---|---|---|---|---|
| ≤ Seven Days | > Seven Days | |||
| 1200 to 2000, g | > 2000, g | 1200 to 2000, g | > 2000, g | |
| Amikacin | 7.5 (Per 12 - 18 hr) | 10 (Per 12 hr) | 7.5 (Per 8 - 12 hr) | 10 (Per 8 hr) |
| Gentamicin | 2.5 (Per 12 - 18 hr) | 2.5 (Per 12 hr) | 2.5 (Per 8 - 12 hr) | 2.5 (Per 8 hr) |
| Ampicillinb,c | 50 (Per 24 hr) | 75 (Per 24 hr) | 75 (Per 24 hr) | 100 (Per 24 hr) |
amg/kg/hr, IM or IV.
bIn meningitis dose of Antibiotics will doubled.
cDoses of Ampicillin were equal in two groups.
2.5. Inclusion and Exclusion Criteria
Infants with indication of treatment with aminoglycoside, whose parents had provided an informed consent, were included in the study. In addition, the exclusion criteria were underlying congenital renal and urinary tract disorders, such as Bartter, RTA and any proximal tubular dysfunction, recent history of nephrotoxic medications use, especially gentamicin and amikacin, ABG acid-base disorders, and disrupted tests before the start of treatment.
2.6. Ethical Considerations
Ethical issues (including plagiarism, data fabrication, and double publication) ware completely taken into consideration by the authors. In addition, the ethical committee of Arak University of Medical Sciences approved the study protocol.
Table 2.
Demographic Status of Children in the Gentamicin and Amikacin Groups
| Variables | Groups | Total | P Value | |
|---|---|---|---|---|
| Gentamicin | Amikacin | |||
| Gender | 0.652 | |||
| Male | 21 (52.5) | 24 (60) | 45 (56.2) | |
| Female | 19 (47.5) | 16 (40) | 35 (43.8) | |
| Age, y | 1 | |||
| Mean ± SD | 3.51 ± 2.76 | 3.22 ± 2.50 | 3.36 ± 2.63 | |
| Fathers education level | 0.864 | |||
| Under diploma | 20 (50) | 21 (52.5) | 41 (51.3) | |
| Diploma and associate | 17 (42.5) | 15 (37.5) | 32 (40) | |
| Bachelor and higher | 3 (7.5) | 4 (10) | 7 (8.7) | |
| Mothers education level | 0.407 | |||
| Under diploma | 24 (60) | 19 (47.5) | 43 (53.8) | |
| Diploma and associate | 14 (35) | 15 (37.5) | 29 (36.2) | |
| Bachelor and higher | 2 (5) | 6 (15) | 8 (10) | |
| Fathers occupation | 0.338 | |||
| Self-employed | 20 (50) | 26 (65) | 46 (57.5) | |
| Employer | 16 (40) | 10 (25) | 26 (32.5) | |
| Employee | 4 (10) | 4 (10) | 8 (10) | |
| Mothers occupation | 0.603 | |||
| Housewife | 39 (97.5) | 38 (95) | 77 (96.3) | |
| Employer | 1 (2.5) | 1 (2.5) | 2 (2.5) | |
| Employee | 0 (0) | 1 (2.5) | 1 (1.2) | |
| Living area | 1 | |||
| Urban | 25 (62.5) | 24 (60) | 49 (61.3) | |
| Rural | 15 (37.5) | 16 (40) | 31 (38.7) | |
Table 3.
Kidney Function Tests and Electrolytes in Gentamicin and Amikacin Groups
| Variables | Groups | Total | P Value | |
|---|---|---|---|---|
| Gentamicin | Amikacin | |||
| Bicarbonate | 0.558 | |||
| Mean ± SD | 17.74 ± 2.39 | 18.13 ± 3.47 | 17.94 ± 2.84 | |
| BUN before treatment, mg/dL | 0.992 | |||
| Mean ± SD | 29.85 ± 14.38 | 29.81 ± 16.33 | 29.83 ± 15.35 | |
| BUN after treatment, mg/dL | 0.670 | |||
| Mean ± SD | 23.45 ± 14.53 | 24.87 ± 15.25 | ||
| GFR before treatment, mL/min | 0.402 | |||
| Mean ± SD | 26.73 ± 7.47 | 29.11 ± 16.24 | 28.41 ± 11.85 | |
| GFR after treatment, mL/min | 0.324 | |||
| Mean ± SD | 41.81 ± 18.28 | 38.21 ± 13.85 | 40.01 ± 16.05 | |
| Cr before treatment, mg/dL | 0.896 | |||
| Mean ± SD | 0.85 ± 0.21 | 0.84 ± 0.26 | 0.85 ± 0.23 | |
| Cr after treatment, mg/dL | 0.340 | |||
| Mean ± SD | 0.56 ± 0.16 | 0.60 ± 0.16 | 0.58 ± 0.16 | |
| Calcium, mg/dL | 0.813 | |||
| Mean ± SD | 8.68 ± 0.7 | 9.11 ± 1.2 | 8.89 ± .0.95 | |
| Sodium, mEq/L | 0.431 | |||
| Mean ± SD | 138.87 ± 5.71 | 139.98 ± 6.8 | 139.58 ± 6.25 | |
| Potassium, mEq/L | 0.158 | |||
| Mean ± SD | 4.42 ± 0.62 | 4.61 ± 0.54 | 4.51 ± 0.58 | |
Table 4.
Delivery and Medical Status of Children in the Gentamicin and Amikacin Groups
| Variables | Groups | Total | P Value | |
|---|---|---|---|---|
| Gentamicin | Amikacin | |||
| Gestational age, week | 1 | |||
| Mean ± SD | 35.4 ± 3.08 | 35.4 ± 5.39 | 35.4 ± 4.23 | |
| Birth weight, g | 0.965 | |||
| Mean ± SD | 2477.25 ± 624.55 | 2470.37 ± 780.19 | 2473.31 ± 702.35 | |
| Infection source | 0.619 | |||
| Sepsis | 33 (82.5) | 35 (87.5) | 68 (85) | |
| Pneumonia | 5 (12.5) | 4 (10) | 9 (11.3) | |
| UTI | 2 (5) | 1 (2.5) | 3 (3.7) | |
| Birth height, cm | 0.237 | |||
| Mean ± SD | 47.52 ± 2.59 | 46.71 ± 3.44 | 47.11 ± 3.01 | |
| Birth head circumference, cm | 0.652 | |||
| Mean ± SD | 33.3 ± 2.08 | 32.77 ± 3.02 | 33.03 ± 2.49 | |
| Type of milk | 0.346 | |||
| Formulas | 0 (0) | 1 (2.5) | 1 (1.2) | |
| Breast milk | 39 (97.5) | 36 (90) | 75 (93.8) | |
| Both | 1 (2.5) | 3 (7.5) | 4 (5) | |
| Multiple pregnancies | 0.317 | |||
| Singleton | 34 (85) | 35 (87.5) | 69 (86.3) | |
| Twins | 4 (10) | 4 (10) | 8 (10) | |
| Triplets | 2 (5) | 1 (2.5) | 3 (3.7) | |
| Gestational diabetes | 1 | |||
| Yes | 5 (12.5) | 5 (12.5) | 10 (12.5) | |
| No | 35 (87.5) | 35 (87.5) | 70 (87.5) | |
| Number of pregnancy | 0.009 | |||
| 1 | 13 (32.5) | 23 (57.5) | 36 (45) | |
| 2 | 12 (30) | 14 (35) | 26 (32.5) | |
| 3 | 12 (30) | 1 (2.5) | 13 (16.3) | |
| > 3 | 3 (7.5) | 2 (5) | 5 (6.2) | |
| Gestational HTN | 1 | |||
| Yes | 1 (2.5) | 1 (2.5) | 2 (2.5) | |
| No | 39 (97.5) | 39 (97.5) | 78 (97.5) | |
| Delivery maternal age, y | 0.235 | |||
| Mean ± SD | 30.30 ± 5.74 | 28.77 ± 5.65 | 29.5 ± 5.70 | |
2.7. Statistical Analysis
Data analysis was conducted by frequency, mean, standard deviation, and standard error, for quantitative variables in the SPSS program. In addition, covariance analysis, chi-square test, independent T-test, or equivalent non-parametric tests were used to compare the mean parameters in groups, and after these tests significant differences (P < 0.05) were considered.
3. Results
A statistically significant difference was found between evaluated factors, thus nephrotoxic effect of Gentamicin and Amikacin were equal in the current study. Based on Table 2, demographic information in the 2 groups were equal. In total, 80 children were evaluated, 45 male and 35 female (P = 0.652). Mean age of children was 3.51 ± 2.76 in the Gentamicin group, 3.22 ± 2.50 in the Amikacin group, and 3.36 ± 2.63 in total (P = 1). Also, other evaluated factors including father’s educational status (P = 0.864), mother’s educational status (P = 0.407), father’s occupation status (P = 0.338), mother’s occupation status (P = 0.603), and living area (P = 1) were equal in the 2 groups. Based on Table 3, that indicated renal function tests criteria, these 2 drugs did not have different nephrotoxic effects on children. Furthermore, BUN before treatment with antibiotics in the gentamicin group was 29.85 ± 14.38 and in the amikacin group was 29.81 ± 16.33 (P = 0.670) and after treatment with antibiotics in the gentamicin group, BUN was 23.45 ± 14.53 and in the amikacin group, it was 24.87 ± 15.25 (P = 0.992). Glomerular Filtration Rate before treatment with antibiotics in the gentamicin group was 26.73 ± 7.47 and in the amikacin group was 29.11 ± 16.24 (P = 0.402), and after treatment with antibiotics, in the gentamicin group, it was 41.81 ± 18.28 and in the amikacin group, 38.21 ± 13.85 (P = 0.324). Before treatment with antibiotics in the gentamicin group Cr was 0.85 ± 0.21 and in the amikacin group, it was 0.84 ± 0.26 (P = 0.896) and after treatment with antibiotics in the gentamicin group, this was 0.56 ± 0.16 and in the amikacin group, it was 0.60 ± 0.16 (P =0.340). Calcium in the gentamicin group was 8.68 ± 0.7 and in the amikacin group was 9.11 ± 1.2 (P = 0.813). Sodium in the gentamicin group was 138.87 ± 5.71 and in the amikacin group was 139.98 ± 6.8 (P = 0.431). Potassium in the gentamicin group was 4.42 ± 0.62 and in the amikacin group was 4.61 ± 0.54 (P = 0.158). Bicarbonate in the gentamicin group was 17.74 ± 2.39 and in the amikacin group, this was 18.13 ± 3.47 (P = 0.558). As shown in Table 4, there were no differences between the 2 groups regarding delivery status of children. In this section, gestational age, birth weight, infection source, birth height, head circumference at birth, type of consumed milk and maternal diseases during pregnancy were evaluated; all of these studied variables were equal in the 2 groups of gentamicin and amikacin (P < 0.05).
4. Discussion
The current study compared nephrotoxic effect of gentamicin and amikacin. It was concluded that based on the current study, the nephrotoxic effect of gentamicin and amikacin were equal and there were not aesthetic preferences for these drugs. Bajracharya et al. in a study compared nephrotoxic effect of amikacin and gentamicin throughout creatinine clearance test, in post-operative patients with normal renal function. They found that although the dose of administered gentamicin is much lower than amikacin, gentamicin has a greater nephrotoxic effect (9), but this study found that nephrotoxic effect of these drugs were equal in the 2 groups. Sweileh et al. in their study investigated the nephrotoxic effect of gentamicin and amikacin. They evaluate 94 children in 2 groups of gentamicin (45 children) and amikacin (49 children). They found that amikacin was significantly less nephrotoxic than gentamicin and that multiple dosing of gentamicin was more nephrotoxic than single dosing, yet the nephrotoxic effect of amikacin was not significantly dependent on frequency of dosing (10); the current study did not confirm these results. Also, Dayan et al. in a study found that nephrotoxic effect were reduced by reduction in frequency of aminoglycosides consumption (11); this factor was not evaluated in the current study. Sassen et al. in a study, evaluated the effect of gentamicin on dysregulation of renal sodium transporters in rats. They found that the fraction excretion of electrolytes was significantly increased in 7 days of treatment with gentamicin (12). Takamoto et al. in a study on the effect of antibiotics on glucose absorption in the kidneys, found that glucose absorption in proximal tubule of kidneys were reduced in children with consumption of gentamicin (13). Akbari et al. in a study investigated the effect of anti-biotherapy on renal function. They evaluated 142 patients and found that GFR contributed to renal function and it was reduced in children treated by antibiotics (14), which is similar to the current findings. Also, Wolf et al. in their study found that impaired renal function was higher in infections of diabetic foot (15). Pannell et al. in a study evaluated nephrotoxic effect of gentamicin and found that gentamicin had some complications on kidneys (16). Roger et al. in a study evaluated the impact of amikacin and gentamicin on the serum concentrations. They conducted this on 63 ICU patients with severe sepsis. Also, these drugs increased peak serum concentrations in 59% of patients (17). Sonia et al. conducted a study on neonates and evaluated fractional excretion of Magnesium, as a marker of nephrotoxicity induced by aminoglycoside, and found that FE of Mg could be considered as a biomarker of tubular damage and nephrotoxicity effect of aminoglycoside therapy could be detected by this marker (18). Therefore, all of the mentioned studies found the nephrotoxicity effect of gentamicin and amikacin and the difference of their complications, yet the current study did not find this difference in nephrotoxicity effect of drugs. The limitation of this study was the lack of cooperation of parents in the study, however after the importance of antibiotherapy on renal function was explained to them, they were convinced. Based on a few clinical studies that have been carried out regarding the nephrotoxic effect of aminoglycoside in children, further studies are required with greater number of cases for evaluation of antibiotic side effects.
4.1. Conclusion
Based on the current study, there are no differences between gentamicin and amikacin regarding nephrotoxic effects. Therefore, there are no aesthetic preferences regarding side effects, between gentamicin and amikacin for use in the pediatrics population.