



1. Background
Renal dysfunction gradually leads to end-stage renal disease (ESRD), the stage of renal failure that requires renal replacement therapy (1). In recent years, the incidence and prevalence rates of ESRD have increased in Iran and globally following a surge in the prevalence of diabetes and hypertension (2). The number of hemodialysis patients has doubled in recent decades, and these patients face a variety of problems (3), such as physical, psychological, and social problems, including cognitive impairment directly related to the fact that a further decline in renal function is associated with the exacerbation of cognitive disorders (4).
In some studies, the prevalence of cognitive impairment in hemodialysis patients was reported to be 30 - 60%, which is about twice that of non-hemodialysis patients (5). In other studies, the prevalence of cognitive impairment was reported to be 50 - 78%, which was higher in ESRD patients than in controls (6). This increase occurs due to various reasons, including uremia, inflammation, cardiovascular disease, stroke, and various metabolic disorders (6, 7). Kidney and brain functions are interrelated, and both organs are affected by the cardiovascular system and blood pressure, and any changes and disorders in kidney function affect brain function as well (8, 9). Kidney dysfunction can be associated with brain dysfunction in various forms, one of which is cognitive disorders (10). Cognitive disorders in dialysis patients are associated with decreased patient cooperation, continuation of dialysis, treatment costs, mortality, and hospitalization of these patients (6). The epidemiological study is the main step to evaluate the clinical impact of cognitive impairment and planning management strategies.
2. Objectives
Given that no study has been conducted in Zahedan, we sought to assess the prevalence and causes of cognitive impairment in hemodialysis patients in Zahedan, Iran, and design a model to predict the amount of cognitive impairment risk.
3. Methods
In this descriptive cross-sectional study, all hemodialysis patients aged less than 60 years old with at least 6 months of hemodialysis at Ali Ibn Abitaleb and Khatam Al-Anbia hospitals were enrolled from April to October 2019 in Zahedan, Iran. The inclusion criteria included patients with no history of known mental illness, psychosis, depression, mental retardation, or stroke. All patients have hemoglobin (Hb) > 10 mg/dL and Kt/V > 1.2 (K, dialyzer clearance of urea; t, dialysis time; V, volume of distribution of urea).
Exclusion criteria included patients with a history of transplant rejection, recent infection (past 3 months) and admission, uncontrolled hypertension, uncontrolled diabetes mellitus, or unwillingness to participate. Finally, 114 patients were enrolled in this study according to the inclusion and exclusion criteria. The Ethics Committee of Zahedan University of Medical Sciences approved this study (code: IR.ZAUMS.REC.1397.62). After obtaining patients' consent, an information checklist, including age, gender, lifetime frequency of hemodialysis, and duration of hemodialysis, was completed by the researcher during interviews with patients. Patients underwent a thorough examination, as well as a neurological examination, by the researcher.
Patients' cognitive function was assessed by the mini-mental state examination (MMSE). Based on the scores obtained on this scale, patients were assigned to one of 3 groups: normal (score 24 and above), suspected of cognitive impairment (score 18 - 23), and cognitive problem (score less than 18). The mini-mental state examination evaluates orientation, registration, calculation, recent memory, visuospatial thinking, and language situation. The reliability and validity of this questionnaire in Iran were proven by Seyedian et al. (Cronbach α = 0.81) (11). The data were analyzed using SPSS version 20 (SPSS Inc, Chicago, Ill, USA).
Chi-square and analysis of variance (ANOVA) were used to analyze the data. The multivariate linear regression test with backward elimination technique was used for the final model predicting the MMSE score. A P-value of less than 0.05 was considered significant.
4. Results
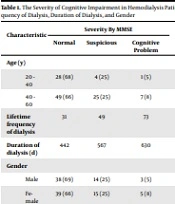
As mentioned above, 114 hemodialysis patients were enrolled in the present study, 48% of whom were male, and 52% of whom were female. Also, 68% had normal cognitive impairment, 25% had suspected cognitive impairment, and 7% had impaired cognitive impairment. The mean age for patients without cognitive impairment was 42 ± 8 years, for suspected patients was 50.7 ± 10 years old, and for patients with problems was 49 ± 10 years old. The results showed a significant relationship between age, lifetime frequency of dialysis, and duration of dialysis (Table 1). There was no significant difference between the 2 sexes in cognitive impairment.
| Characteristic | Severity By MMSE | P-Value | ||
|---|---|---|---|---|
| Normal | Suspicious | Cognitive Problem | ||
| Age (y) | ||||
| 20 - 40 | 28 (68) | 4 (25) | 1 (5) | 0.000 |
| 40 - 60 | 49 (66) | 25 (25) | 7 (8) | |
| Lifetime frequency of dialysis | 31 | 49 | 73 | 0.003 |
| Duration of dialysis (d) | 442 | 567 | 630 | 0.000 |
| Gender | ||||
| Male | 38 (69) | 14 (25) | 3 (5) | 0.067 |
| Female | 39 (66) | 15 (25) | 5 (8) | |
The Severity of Cognitive Impairment in Hemodialysis Patients by Age, Frequency of Dialysis, Duration of Dialysis, and Gender
Considering that cognitive disorders had a significant relationship with age and duration, and frequency of dialysis. According to the obtained results, we found this model to predict the MMSE score, which can be predicted by these items according to the formula obtained (MMSE score = 35.33 - [0.429 × age] - [0.336 × dialysis duration] - [0.239 × dialysis time]).
Based on the multivariate linear regression test by the backward method, the final model predicting the MMSE score is summarized in the Table 2. As can be seen, this model predicts 0.47% of the MMSE variance, and the prediction coefficient of each variable in the regression model (beta) is summarized in Table 2.
| Parameter | B | SE | Beta | t | P-Value |
|---|---|---|---|---|---|
| Constant | 35.33 | 1.26 | - | 27.89 | 0.000 |
| Age | -0.148 | 0.024 | -0.429 | -6.19 | 0.000 |
| Dialysis duration | -0.052 | 0.011 | -0.366 | -4.66 | 0.000 |
| Lifetime frequency | -0.005 | 0.002 | -0.239 | -3.02 | 0.003 |
Results of Multivariate Regression Analysis to Predict the MMSE Score
5. Discussion
The results of this study showed that cognitive disorders were common in hemodialysis patients, and about one-third of these patients had cognitive impairment, which was clearly higher than the rate in the general population (3.2%) (12). The results of our study are in line with the results of other studies, such as in the United States that the population of hemodialysis patients is 700,000, two-thirds of whom have cognitive impairment (13). Other studies have also reported a high prevalence of cognitive impairment in ESRD patients. Eslami Amirabadi et al. in a study performed in Tehran reported this rate to be 47% (9). Kalirao et al. found that two-thirds of hemodialysis and peritoneal dialysis patients had cognitive impairments, which is consistent with our finding if we consider the total number of suspected and problematic cases (7); also, it is consistent with the results of Tamadon et al., who showed that 28.2% of ESRD patients had severe cognitive impairment, which was significantly higher than the rate of cognitive impairment in patients with chronic kidney disease (14). Murray et al. reported that more than one-third of hemodialysis patients had severe cognitive impairment (15); this high prevalence can have several causes. For instance, kidney problems can affect brain function. Aging, diabetes mellitus, hypertension, hypercholesterolemia (along with chronic inflammation), oxidative stress, and hypercoagulopathy can also cause vascular and endothelial damage, affecting the kidneys and the brain. Uremic toxins have a direct effect on neurons through the neurodegenerative mechanism (10).
Further, studies have shown that dialysis patients have brain atrophy, reduced hippocampal volume, thinning of the cerebral cortex in the temporomandibular joint and white matter damage in the fornix, inner capsule, and thalamus, all of which are similar to aging changes. This evidence can be seen on imaging even before changes the hemodialysis patient's functional and cognitive status (16). On the other hand, chronic inflammation in hemodialysis patients increases the level of cytokines, impairs the secretion of neurotransmitters, and exacerbates neurological and cognitive disorders (17). Studies have also demonstrated that decreased cerebral blood flow during dialysis and continued dialysis during the month are associated with cerebrovascular disease and decreased cerebral function in these patients (18). In general, the common mechanisms of increased cognitive impairment in hemodialysis patients increase by vascular disease, oxidative stress, silent or overt cerebral infarction, hyperhomocysteinemia, impaired renal function, anemia, inadequate dialysis, malnutrition, and chronic inflammation (10).
Our study indicated that the increased frequency of dialysis and the number of years of dialysis were associated with a higher rate of cognitive impairment. The results were consistent with the results obtained by Sarnak et al., as well as the hypothesis that an increase in the speed of atherosclerosis is associated with a higher MMSE score (19). Studies have shown that brain function improves following kidney transplantation (18), and efforts should be made to provide kidney transplantation for these patients more quickly. The rate of cognitive disorders in hemodialysis patients is high due to the increased prevalence of diabetes and hypertension, followed by renal dysfunction and increased need for dialysis, and these patients need special care. Cognitive impairment is associated with increased mortality and hospitalization (13). According to our model, elderly patients who have been dialyzed longer and patients who have been on dialysis more often are at a higher risk for cognitive impairment. Other studies confirm our results (19). It is recommended that during periodic visits of hemodialysis patients, these patients should be examined for cognitive impairment and, if necessary, treatment should be initiated as soon as possible, and, if possible, kidney transplantation should be performed more quickly.
Moreover, the small number of samples and the lack of imaging, along with not examining the inflammatory factors, were the limitations of our study.
