




1. Background
The increasing prevalence of chronic diseases has become a major problem in developed as well as developing countries (1). Chronic diseases, with cardiovascular diseases (CVDs), cancer, diabetes, and chronic respiratory diseases as the major ones, claimed more than 30 million lives worldwide in 2008 (2) and have become the leading cause of death in many countries. While CVDs are declining in developed countries, they are not only a major cause of death in developing countries but also have become a significant public health concern due to their rising trend. Today, coronary heart disease is the most common cause of mortality worldwide and is predicted to be the most important cause of global death by 2030 (3, 4). Cardiovascular mortality is also the most common cause of death in Iran, with the highest mortality rate (3, 5).
Congestive heart failure often referred simply to as heart failure, is the underlying cause of more than 55,000 deaths each year, with one out of every nine deaths occurring annually (3, 6). Heart failure is a debilitating condition caused by an inherited or acquired disorder in the structure or function of the heart and has profound effects on patients’ functional conditions and quality of life (6, 7). The disease is often progressive, in which the heart is unable to supply sufficient blood to meet the metabolic needs of organs and tissues. It also reduces the capacity for physical activities and causes short breathing (8). About half of patients with heart failure die after being hospitalized or are at increased risk of re-admission (9). The disease and its consequences cost the health care sector a great deal. In the United States, for example, such cost is estimated at more than 20 billion dollars (10). The cost was estimated to be 400 million dollars in Iran in 2007 (11). The prevalence of CVDs is 2 - 3%, increases with age, and is higher in men than women (12, 13).
Cardiovascular drugs lead to oral complications in 14% (14) to 67.4% (15) of patients. Angiotensin-converting enzyme inhibitors (aceis) can cause oral lichen planus, burning mouth sensation, and ageusia (16). Lichenoid reactions have also been described in association with alpha- and beta-adrenergic blockers. Taste perception abnormalities may also be caused by aspirin, statins, and diuretics (17).
2. Objectives
The goal of treating heart failure is to alleviate symptoms, improve patients’ functional conditions and quality of life, increase survival, and achieve disease adaptation. There are many medications prescribed for heart failure, including angiotensin-converting enzyme inhibitors, beta-blockers, diuretics, and digitalis. Due to the increasing trend of using heart failure medications, the side effects of these drugs are expected to increase further. Therefore, specialized preventive and therapeutic care are necessary today more than ever. The aim of this study was to evaluate the oral side effects of heart failure drugs in patients with congestive heart failure.
3. Methods
In this cross-sectional study, 340 patients referring to heart clinics in the city of Birjand, Iran, from March to September 2016, who had heart failure treated with heart failure medication were included. Those receiving concomitant medications for diabetes, hypothyroidism, and hyperthyroidism, as well as patients with dementia, confusion, and physical disabilities, were excluded (14).
Written informed consent was obtained from all participants before entering the study and after a comprehensive introduction to the study protocol. Patients were divided into four groups according to the type of medication used to treat heart failure, as follows: (1) Angiotensin receptor blockers (ARB), (2) angiotensin receptor blockers + beta blockers (ARB + BAB), (3) beta-blockers + nitrates + antiplatelet + angiotensin receptor blockers or angiotensin-converting enzyme inhibitors (BAB + Nitrate + Anti Plt + ARB or ACEI), (4) digoxin + diuretics + angiotensin receptor blockers or angiotensin-converting enzyme inhibitors (Digital + dieuretics + ACEI or ARB).
Data on demographic characteristics, number of medications and duration of use, hospitalization, and medical records were collected. A complete history of oral symptoms, such as oral dryness, changes in taste or burning sensation in the mouth, and other symptoms, were also asked orally according to a standard checklist by the examiner. Moreover, a full clinical examination of the oral cavity for the presence of any oral mucosal lesions was performed using a mirror and dental probe. Data analysis was administered using SPSS version 22 by the chi-squared and the ANOVA. Descriptive information are provided using frequency tables. Statistical significance was considered when the P-value < 0.05.
4. Results
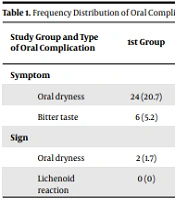
This study was performed on 340 patients (146 men (42.9%) and 194 women (57.1%)) with heart failure referring to heart clinics in the city of Birjand in Iran in 2016. The youngest and oldest participants were 32 and 86 years old, respectively, with a mean age of 60.13 ± 9.35 years. Most patients were using angiotensin receptor blocking drugs (n = 116; 34.1%). The frequency distribution of patients according to their education level were as follows; 19.7% were illiterate (67 patients), 42.05% had lower secondary education (143 patients), 23.5% with high school diploma (80 patients), and 14.7% with higher educations (50 patients). Oral complications of heart failure medications were evaluated, including oral dryness, bitter taste in the mouth, lichenoid reaction, gingival enlargement, burning sensation, oral aphthous, angioedema, facial lupus, lymphadenopathy, petechia, oral ulcer, and high salivation. According to Table 1, the highest frequency of oral complications was observed in patients taking beta-blocker + antiplatelet + angiotensin-blocking drug or angiotensin enzyme inhibition. The most common complication was oral dryness, followed by bitter taste in the mouth. There was also a significant relationship between oral dryness, bitter taste in the mouth, and the type of medication used (P < 0.05).
| Study Group and Type of Oral Complication | 1st Group | 2nd Group | 3rd Group | 4th Group | Total | Statistical Test Results | |
|---|---|---|---|---|---|---|---|
| P | χ2 | ||||||
| Symptom | |||||||
| Oral dryness | 24 (20.7) | 28 (24.3) | 43 (47.3) | 3 (16.7) | 98 (28.8) | < 0.001 | 21.2 |
| Bitter taste | 6 (5.2) | 11 (9.6) | 20 (22) | 6 (5.6) | 38 (11.2) | < 0.001 | 10.8 |
| Sign | |||||||
| Oral dryness | 2 (1.7) | 9 (7.8) | 14 (15.4) | 2 (11.1) | 27 (7.9) | 0.004 | 13.3 |
| Lichenoid reaction | 0 (0) | 2 (1.7) | 4 (4.4) | 0 (0) | 6 (1.8) | 0.11 | 5.11 |
Frequency Distribution of Oral Complications of Heart Failure Drugs in Patients Referred to Birjand Heart Clinics in 2016 by Medication Group a
There was also a significant relationship between oral dryness, bitter taste in the mouth, and the duration of drug use (P < 0.05). On the other hand, there was no significant relationship between lichenoid reaction time and the duration of drug use (P > 0.05). The most common complication was in patients with a history of over 5 drug use. Oral dryness was more common in females than males, and no significant relationship was found between complications and gender (P > 0.05).
According to Table 2, the mean age and the duration of drug use in patients with drug side effects were significantly higher than that of those receiving heart failure medications (P < 0.001). As shown in Table 3, there was a significant difference between the prevalence of side effects depending on the duration of drug use and age. The prevalence of drug side effects was significantly enhanced with the increase in the duration of drug use and age (P < 0.001).
| Drug Complication Status/Variable | Present (n = 188) | Absent (n = 188) | Independent t-Test Results |
|---|---|---|---|
| Age (y) | 66.0 ± 8.61 | 57.6 ± 8.5 | t = 8.381; df = 338; P < 0.001 |
| Duration of drug use (y) | 7.29 ± 3.1 | 3.72 ± 1.62 | t = 14.016; df = 338; P < 0.001 |
Comparison of Mean Age and Duration of Drug Use According to Different Oral Drug Complications in Patients a
| Drug Complication Status/Variable | Present | Absent | χ2-Test Results |
|---|---|---|---|
| Duration of drug use (y) | χ2 = 108.5; df = 2; P < 0.001 | ||
| < 4 | 11 (8.5) | 119 (91.5) | |
| 4 - 6 | 20 (19) | 85 (81) | |
| > 6 | 72 (68.8) | 33 (31.4) | |
| Gender | χ2 = 1.29; df = 1; P < 0.26 | ||
| Male | 49 (33.6) | 97 (66.4) | |
| Female | 54 (27.8) | 140 (72.2) | |
| Age (y) | χ2 = 73.4; df = 2; P < 0.001 | ||
| < 50 | 4 (10.8) | 33 (89.2) | |
| 50 - 65 | 33 (16.8) | 163 (83.2) | |
| > 65 | 66 (61.7) | 41 (38.3) |
Comparison of Prevalence of Drug Side Effects According to Age, Gender and Duration of Drug Use a
5. Discussion
The most common drug side effect was observed in those older than 65, which was not unexpected due to the high prevalence of CVDs in these ages. Moreover, the most common complications and manifestations were observed in female patients. It could probably be due to the fact that women, in general, undertake more medical visits than men, leading to higher rates of reporting hypertension in women in most studies. Thirty percent (103 out of 340) of patients with heart failure taking medications had oral manifestations and complications.
Habbab et al. reported a prevalence of 14.1% for these complications (14). In another study by Arunkumar et al., 382 (out of 603) patients with hypertension (63.3%) had at least one manifestation and oral side effects of antihypertensive drugs (15). The most common complication observed in this study was oral dryness (n = 98; 28.8%), which is in agreement Shinkai et al. and Smith and Burtner (18, 19).
Mohan et al. reported a prevalence of 50% for oral dryness (20). Bitter taste in the mouth (n = 20; 7.9%) has also been reported as the second common oral manifestation (after oral dryness), with the highest prevalence in the third group of drug users (BAB + Nitrate + anti-Plt + ARB or ACEI) (n = 14; 15.4%). Luzardo and Raad Bassil (21) reported that 80.53% of patients using antihypertensive drugs had oral manifestations. The most common manifestation was dysgeusia (60%), followed by hyposalivation (58%) and gingival enlargement (12%), which is not consistent with our study. The results of this study are consistent with Arunkumar et al., who reported oral dryness as the most common oral complication (n = 10; 6.6%), followed by bitter taste in the mouth (n = 3; 2.8%) (15).
In the present study, the frequency of lichenoid reaction in patients was 1.8% (6 cases). The results are consistent with Arunkumar et al., which stated that the most common oral complication in patients taking the calcium channel blocker drug was oral dryness (n = 29; 19.1%). However, our findings are not consistent with respect to the frequency of gingival enlargement, which was 18 cases (33.3%) (15). According to Mohan et al., the most common complication next to oral dryness is oral hyperpigmentation (23.3%) (18). Arunkumar et al. reported that the most common complications in this group of patients were oral dryness (n = 19) and oral bitterness (n = 18; 16.8%) (15).
In the present study, gingival enlargement was observed in six cases (1.8%), four of which (4.4%) were in patients taking the third drug (BAB + Nitrate + anti-Plt + ARB or ACEI). It is consistent with Arunkumar et al. (15), stating that the most common complication in this group was oral dryness, bitter taste in the mouth, and lichenoid reaction with a frequency of four (14.8%), respectively.
The oral dryness complication of the drugs used in CVDs roots in their anticholinergic effects. Many studies showed that the prevalence and incidence of oral dryness increase with age. Other causes may include aging, gender, dehydration, habits such as oral breathing, smoking, alcohol consumption, decreased salivary gland function, salivary gland diseases (e.g., sialolite, sialadenitis, and sjogren’s syndrome), stress, depression, and systemic diseases such as diabetes and hypertension (22). The bitter taste in the mouth may be due to decreased salivary flow or the secretion of drugs into the saliva, leading to a change in the taste.
Some studies suggested that certain drugs used to treat heart disease lead to changes in the perception of food taste (15). There is evidence that drugs can influence the taste of foods by affecting the metal ions associated with cell membranes. In the present study, some complications and lesions, such as gingival enlargement, oral aphthous ulcer, oral ulcer, high salivation, petechia, lymphadenopathy, lupus lesions, and facial angioedema, were not observed in any patient. In the study by Habbab et al., the prevalence of any of the complications ulcers, lichenoid reaction, oral aphthous, and burning sensation was less than 1% (14).
5.1. Conclusions
This study demonstrated an increased prevalence of side effects related to CVD drugs. It can be attributed to factors like increased life expectancy, resulting in prolonged consumption of drugs, and increased prevalence of the diseases. These complications could also be oral, and dentists might, therefore, play a crucial role in reducing such complications. It appears that defining protocols to visit dentists as well as informing cardiologists and patients about the beneficial role of the dentist in reducing oral complications can be highly advantageous.
5.2. Limitations
We did not consider the personal dental hygiene of patients (as an interfering factor) in the study.
