


1. Background
The mechanism of NVD involves the flexed head of the giving birth fetus, which is engaged so that the fetal occiput is placed near one of the lateral edges of the mother's pelvis at the onset of labor. With the progress of labor, progressive flexion and descent of the fetus make the occiput, when it reaches the pelvic floor, turns anteriorly. When one of the steps goes wrong, malposition and malpresentation happen. The term "presentation" refers to the part of the fetus that is presented at the inlet of the pelvis or the part of the fetus that occupies the lower segment of the uterus. Approximately 95% of the fetuses present with vertex at term. The rest of the presentations, which are classified as malpresentation.
The position is referred to as the relationship between the denominator and the points in the mother's pelvis, such as symphysis pubis, sacroiliac joints, and sacrum. For vertex presentation, the occiput can be placed in the following positions: Occiput anterior (OA), occiput transverse (OT), and occiput posterior (OP) (1). The position of the fetal head during labor is usually determined by finger examination. Touch of sagittal sutures and fontanels determines the position of the occiput with the mother pelvis (1, 2). About 10% of all pregnancies occur with malposition and malpresentation, and this is a challenge for obstetricians. These are well-known causes of failure to progress (2).
Ultrasound is a non-invasive procedure and seems to be more accurate than finger examination in determining the position of the fetal head. Careful evaluation of the fetal occiput position during delivery, especially in operative vaginal delivery, is of particular importance (3, 4).
Various studies have compared ultrasound and finger examination to determine the position of the fetal occiput and have reported different results (5-7).
2. Objectives
The aim of this study was to compare abdominal ultrasound with vaginal finger examination to determine position and presentation of fetal head.
3. Methods
This is a descriptive-analytical study that was carried out in Ali ibn-e Abitaleb Hospital of Zahedan in 2018. The purpose of this study was to compare the abdominal ultrasound with finger examination in diagnosis of malposition and malpresentation of fetal head. Inclusion criteria were term pregnancy and the onset of labor (regular and painful contractions), and exclusion criteria were multiple pregnancies, any previous gynecological surgery, preeclampsia, premature rupture of membranes for more than 36 hours, attempted vaginal delivery after cesarean section (VBAC), and fetal distress.
After approving the plan in the Medical School Research, the researcher referred to the delivery ward of Ali ibn-e Abitaleb Hospital of Zahedan, and 100 women were included in the study from April 2018 to October 2018. After obtaining written and oral informed consent, all women underwent vaginal finger examination in the first phase of delivery, and finger examination was performed using classical method with touching of sagittal suture and fontanels and their relation to the mother's pelvis to determine the position of the fetal head.
The position of the fetal head was divided into OA (left or right), OP (left or right), and OT (left or right).
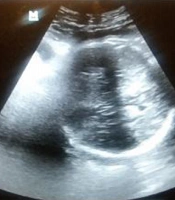
Fetal presentation was also determined by Leopold maneuvers, or finger examination (if cervix will be dilatated); then the information of each patient was recorded electronically, and the patient underwent transdermal ultrasound by authors who were unaware of finger examination results. To determine the position of the fetal head (Figures 1 - 3), the ultrasound transducer was transversely positioned in the suprapubic area of the mother's abdomen, and then the fetal spine was positioned at its sagittal surface and followed from the thorax to the fetal occiput. Positioning was performed by showing intracranial midline structures, if fetal orbits are toward the transducer, posterior occipital position will be detected, if fetal orbits are away from transducer, it will be anterior occiput and anterior and posterior orbits in unilateral of mother represent transverse occiput positions. Finger examinations of all women were performed by a single gynecology assistant, and all ultrasounds were performed by an author with an ultrasound device (Philips).
.")
Ultrasound showing the position of occiput anterior (OA).
.")
A, B, ultrasound showing the position of occiput posterior (OP).
.")
Ultrasound showing the position of occiput transverse (OT).
3.1. Data Analysis
Data were analyzed using SPSS software version 21. The level of agreement between sonography with transvaginal digital examination in the diagnosis of malposition and cephalic malpresentation was analyzed by Cohen’s kappa statistics. When assessing the kappa test, a result > 0.900 was interpreted as almost perfect, 0.800 - 0.900 as strong agreement, 0.600 - 0.790 as moderate agreement, 0.400 - 0.590 as weak agreement, and 0.200 - 0.390 as minimal agreement.
This study was approved by the Ethics Committee of Zahedan University of Medical Sciences with ethics code IR.ZAUMS.REC.1397.150.
4. Results
In this study, 100 pregnant women were studied in the first phase of pregnancy. The mean age of the subjects was 24.7 ± 5.5 years. Moreover, 46% of patients were nulliparous, and 54% were multiparous (gravid mean and other demographic characteristics are listed in Table 1), the rest of the demographic characteristics are listed in Table 1.
| Variables | Mean | Standard Deviation | Minimum | Maximum |
|---|---|---|---|---|
| Maternal age (y) | 24.7 | 5.5 | 16 | 37 |
| Gestational age (weeks) | 39.2 | 1.35 | 36 | 42 |
| Gravidity | 2.41 | 1.89 | 1 | 8 |
Demographic Characteristics of the Participants
In this study, fetal head position was determined by finger examination in 81% of cases and with sonography in 93% of cases. In the 81 fetal head positions determined by digital finger examination, the agreement with ultrasound was weak (Kappa = 0.416) (Table 2). In this study, fetal presentation was detected by finger examination in 93% of cases and by sonography in 100% of cases. The agreement was moderate between ultrasound and digital VE in the population with fetal presentation (Kappa = 0.783) (Table 3).
5. Discussion
Abnormal positions and presentations occur in about 10% of all pregnancies and are challenges for obstetricians. These are well-known causes of failure of progress and usually lead to prolongation or stopping the second phase of delivery. These complications require operative vaginal delivery and increase the likelihood of maternal and fetal complications (8-10).
The aim of this study was to compare finger examinations and abdominal ultrasound in determining fetal position and presentation.
A total of 100 pregnant women who were referred to Ali ibn-e Abitaleb Hospital for delivery were evaluated in this study. The findings showed that the agreement with ultrasound was weak in the 81 fetal head positions determined by digital finger examination, while the agreement between ultrasound and digital VE was moderate in the population with fetal presentation (study of Akmal et al. in England in 496 singleton pregnancies revealed that ultrasound in 100% of cases and finger examination in 67.5% of cases could detect fetal head position that 49.4% of finger examination findings was consistent with ultrasound. They finally concluded that finger examination could not determine the position of the fetal head in more than half of cases (5).
Zahalka et al. in Israel in 60 pregnant women in the second phase of labor reported transient vaginal ultrasound in 100%, abdominal ultrasound in 85%, and vaginal finger examination in 88.3%. The fetal head was diagnosed (6). Chou et al. in the United States, in a study of 88 women in the second phase of labor, reported that finger examination in 71.6% of cases and ultrasound in 92% of cases were able to accurately determine the position of the occiput (7).
In another study, Chan et al., in 2015 in China, compared finger vaginal examination with transdermal abdominal ultrasound to determine the position of the fetal head and studied 100 term mononuclear fetuses with cephalic presentation. They reported that finger examination was consistent with ultrasound in 34% of cases (8). The differences in the results of different studies may be attributed to differences in the demographic characteristics of the subjects studied, stage of delivery, fetal weight, and cervical dilatation rate (9-16). Also, since vaginal finger examination and ultrasound depend on the skill of the examiner and sonographer, this may be another reason for the differences in the results of different studies.
