

1. Background
New technologies have dynamically developed in dentistry as a branch of medicine, allowing dentists to perform more procedures year after year using modern techniques. Many of these technologies have proven effective in improving dental operations and accelerating related strategies. Some of these technologies were introduced to dentistry years ago (1). For example, in 1999, Lussi et al. presented the DIAGNOdent system (KaVo, Biberach, Germany) for detecting and quantifying caries on occlusal surfaces (2). In the early 1970s, Takuo Aoyagi validated pulse oximetry, and in 2007, Gopikrishna et al. developed a pulse oximeter dental probe to evaluate pulp vitality (3).
In 1997, Milestone Scientific Inc. introduced a computer-controlled local anesthetic delivery system (CCLAD) known as the Wand (4). Digital dental education has expanded into five key areas: Digital surface mapping, web-based knowledge transfer and e-learning, digital radiography, dental simulator motor skills (including intraoral optical scanning), and studies on the penetration and acceptance of digital education (5).
Digital radiography offers several benefits, such as exposing the patient to a lower radiation dose and providing immediate diagnostic information, which improves clinical care. Patients perceive significant value in not having to return for a follow-up appointment to receive results. This technology allows for more efficient use of time and resources (6).
Duret first introduced dental computer-aided design/computer-aided manufacturing (CAD/CAM) technology (2). Moermann was the second developer of the CEREC® system, which allowed for the construction of same-day ceramic restorations at the patient's chairside in a dental office. This innovation quickly popularized the term CAD/CAM in dentistry (2).
Today, digital impressions, direct intraoral scanning, or indirect digitization of casts from conventional impressions can create a stereolithography (STL) file, representing the first step in the digital workflow (7). This allows for a virtual 'working cast-free' situation. Nevertheless, when necessary, casts can still be built from the same STL files using rapid prototyping technologies (8).
Intra-oral digital scanners (IOS) have ushered dentistry into a fully digital era, increasing efficiency in several aspects. These scanners eliminate the need for impression trays and materials, which must be disinfected and transferred to the laboratory. Digital files can be forwarded and stored electronically, saving time, cost, and space. Furthermore, the use of IOS reduces distortion and volumetric variations associated with impression materials and die stone properties, decreasing impression time, patient discomfort, and the risk of gag reflex, while improving patient acceptance (9).
While the adoption of these scanners in dental offices is still limited (estimated at 20% - 25% of European dental offices), more than two-thirds of dental laboratories are believed to use laboratory scanners (5). Compared to waxing, digital design offers several advantages for technicians, such as better control over modality, preparation of material thickness data, and values of connector cross-sections. Traditional lost wax casting techniques often resulted in inaccurate castings or shrinkage cavities, whereas a digital workflow improves material properties when using industrial milling or additive printing processes (9).
However, in practice, dental CAD/CAM technology is not always straightforward. The total cost, operation time, and handling of the systems for processing dental devices must match or surpass conventional methods to replace traditional restorations effectively and ensure that these new systems are practical for daily laboratory work and clinical practice. The morphology of the abutment teeth, related adjacent teeth, and opposing teeth must be accurately digitized before designing the restoration. It was challenging to recognize the delicate margin prepared by dentists using the compact digitizers available at the time. Therefore, developing an accurate and compact digitizer with sophisticated software was necessary for high-precision digitizing (2). Moreover, the size of the machine had to be suitable for installation in a standard dental laboratory office (2).
Digital smile design (DSD) is a versatile tool with many advantages, such as facilitating communication between the dentist, patients, and dental technicians, minimizing errors and misunderstandings that could affect the final result, improving diagnosis, pre-operative planning, and the design of aesthetic dental rehabilitations. It also facilitates and speeds up aesthetic treatment planning and provides numerous opportunities for teaching, learning, and routine practice (10-13).
Virtual reality technology is expected to play a dominant role in the future of dental education. However, one of the biggest challenges in digital education is the continuous need to adapt to technological developments and apply these advancements to dental practice (5).
Several studies have explored the level of computerization in dental practices (14-16), the use of computerization for information seeking (5, 17), and the distribution of specific technologies among dental professionals (18, 19). Common technologies in dentistry include digital radiographs, oral scanners, CAD/CAM, 3D printing, electronic patient records, electronic patient referrals, and other dental office communications (20).
Despite substantial evidence supporting the importance of digital technologies, there remains no comprehensive and coherent view of the extent of their use and the factors influencing their adoption in any particular society. Therefore, investigating the extent to which digital technologies are used, the associations they have, and assessing the personal and operational characteristics associated with digital technology adoption is crucial.
2. Objectives
This study aimed to investigate the use of digital technologies among dentists in Zahedan, Iran, in 2023.
3. Methods
This cross-sectional (descriptive-analytical) study was conducted after obtaining approval from the Ethics Committee of Zahedan University of Medical Sciences, Iran (IR.ZAUMS.REC.1401.390). The questionnaire used for this study was adapted from a translated article (21) with some modifications. The reliability of the questionnaire was confirmed at 100%, and the validity was measured at 0.8. The questionnaires were distributed among general and specialized dentists in Zahedan, Iran.
After obtaining written consent from the participants, the questionnaires were administered. A total of ninety-three completed questionnaires were collected from dentists who were willing to participate in the study. The questionnaire consisted of four parts:
The first part included:
- Demographic information (gender, experience, workplace, level of degree).
- Type of education.
- Extent of education in digital dentistry (Not at all, Somewhat, Completely).
The second part, focused on administrative and communicative questions, comprising four questions related to:
- Information collection software for filing patient records and managing the clinic.
- Information websites for scheduling appointments and sending reminders.
- Communication software with other centers, including radiology, insurance, laboratories, and other medical facilities.
- Social networks for informing patients and reminding them of appointments.
The third part, covered clinical and diagnostic questions, consisting of nine questions related to:
- Intraoral digital radiography.
- 3D digital radiography (CBCT).
- Oral cameras.
- Intraoral scanners.
- CAD/CAM systems.
- Digital color determination.
- Smile design software.
- 3D printers.
- Digital microscopes.
The answers to the fundamental questions of the questionnaire were either "Yes" or "No." For each "Yes" response, one point was assigned, and for each "No" response, zero points were given. The usage of various types of technology was classified as follows:
- Low usage: 0 - 3 points.
- Moderate usage: 4 - 8 points.
- High usage: 9 - 13 points.
Based on the responses, additional questions were formulated:
- For questions with a "Yes" answer, two more series of questions were asked regarding the level of satisfaction with the technology (Complete, Intermediate, Lack of satisfaction) and the year of starting to use the technology (Before 2014, 2015 to 2018, After 2019).
- For questions with a "No" answer, the reasons for not using the technology were explored, with options such as No need, Expensive, Time-consuming, Lack of training, and Inaccessibility.
3.1. Data Analysis and Description Method
After collecting the information, the data were entered into SPSS software version 24. In the first step, data quality was checked using graphical methods and calculating descriptive indices. Data frequency analysis and group comparisons were conducted using the chi-square or Fisher's exact test. In all analyses, a P-value of less than 0.05 (P < 0.05) was considered statistically significant.
4. Results
The statistical population of this study consisted of 93 participants, including 44 females and 49 males.
According to Table 1, 60.2% of participants were categorized as low usage, 35.5% as moderate usage, and 4.3% as high usage of digital technologies.
| Rate of Usage | No. (%) |
|---|---|
| Low usage | 56 (60.2) |
| Moderate usage | 33 (35.5) |
| High usage | 4 (4.3) |
| Total | 93 (100) |
Frequency of Use of Digital Technologies by Dentists of Zahedan, Iran
As shown in Table 2:
| Variables | Total | Low | Moderate | High | P-Value |
|---|---|---|---|---|---|
| Gender | < 0.001 | ||||
| Male | 49 (52.68) | 20 (40.8) | 25 (51) | 4 (8.2) | |
| Female | 44 (47.32) | 36 (81.8) | 8 (18.2) | 0 (0) | |
| Experience | < 0.006 | ||||
| 1 - 4 years | 36 (38.8) | 20 (55.6) | 12 (33.3) | 4 (11.1) | |
| 4 - 10 years | 24 (25.8) | 24 (100) | 0 (0) | 0 (0) | |
| More than 10 years | 33 (35.4) | 12 (36.4) | 21 (63.6) | 0 (0) | |
| Work place | < 0.001 | ||||
| Private office or clinic | 69 (74.1) | 32 (46.4) | 33 (47.8) | 4 (5.8) | |
| University or general clinic | 8 (8.6) | 8 (100) | 0 (0) | 0 (0) | |
| Both cases | 16 (17.3) | 16 (100) | 0 (0) | 0 (0) | |
| Level of degree | 0.229 | ||||
| General dentist | 58 (62.3) | 11 (18.9) | 31 (53.4) | 16 (27.7) | |
| Specialist dentist | 35 (37.7) | 4 (11.4) | 25 (71.4) | 6 (17.2) | |
| Amount of education | < 0.002 | ||||
| Not at all | 18 (18.0) | 13 (75) | 5 (25) | 0 (0) | |
| Somewhat | 40 (43.8) | 29 (71.8) | 11 (28.2) | 0 (0) | |
| Completely | 35 (38.2) | 12 (35.3) | 19 (52.9) | 4 (11.8) |
Compare the Frequency of Use of Digital Technologies by Dentists According to Gender, Experience, Workplace, Level of Degree and Amount of Education a
- The chi-square test demonstrated a significant relationship between the use of digital technologies and gender (P < 0.001). Specifically, 40.8% of men and 81.8% of women were classified as low usage.
- The results indicated a significant relationship between the use of digital technologies and experience (P < 0.006). Dentists with 1 - 4 years of experience had higher usage than those with more years of experience.
- Fisher's exact test showed a significant relationship between digital technology usage and workplace (P < 0.001). Participants working in a private office or clinic reported 46.4% low usage, 47.8% moderate usage, and 5.8% high usage.
- The chi-square test results showed no significant relationship between the use of digital technologies and the level of degree (P = 0.229).
- Fisher's exact test concluded a significant relationship between the use of digital technologies and the amount of education (P < 0.002), indicating that dentists with complete education in digital technologies used them more than others.
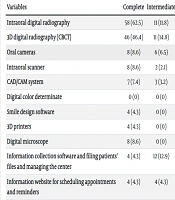
According to the results in Table 3, the most commonly used technology by participants was "Intraoral digital radiography," while the least used was "Digital color determinate." Among those who used intraoral digital radiography, 62.5% reported complete satisfaction with the technology. Most participants began using this technology between 2015 and 2018. Details on the satisfaction levels and the period of using each technology are provided in Table 3.
| Variables | Level of Satisfaction | Year of Starting | ||||
|---|---|---|---|---|---|---|
| Complete | Intermediate | At All | Before 2015 | 2015 - 2018 | After 2019 | |
| Intraoral digital radiography | 58 (62.5) | 11 (11.8) | 0 (0) | 15 (16.1) | 34 (36.7) | 20 (21.5) |
| 3D digital radiography (CBCT) | 46 (46.4) | 11 (14.8) | 0 (0) | 10 (10.7) | 20 (21.5) | 27 (29) |
| Oral cameras | 8 (8.6) | 6 (6.5) | 0 (0) | 3 (3.2) | 4 (4.3) | 7 (7.4) |
| Intraoral scanner | 8 (8.6) | 2 (2.1) | 0 (0) | 2 (2.1) | 3 (3.2) | 5 (5.3) |
| CAD/CAM system | 7 (7.4) | 3 (3.2) | 0 (0) | 2 (2.1) | 3 (3.2) | 5 (5.3) |
| Digital color determinate | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) |
| Smile design software | 4 (4.3) | 0 (0) | 0 (0) | 1 (1.1) | 1 (1.1) | 2 (2.1) |
| 3D printers | 4 (4.3) | 0 (0) | 0 (0) | 1 (1.1) | 2 (2.1) | 1 (1.1) |
| Digital microscope | 8 (8.6) | 0 (0) | 0 (0) | 0 (0) | 3 (3.2) | 5 (5.3) |
| Information collection software and filing patients' files and managing the center | 4 (4.3) | 12 (12.9) | 0 (0) | 4 (4.3) | 4 (4.3) | 8 (8.6) |
| Information website for scheduling appointments and reminders | 4 (4.3) | 4 (4.3) | 0 (0) | 0 (0) | 4 (4.3) | 4 (4.3) |
| Communication software with other centers including radiology, Insurance, laboratories and other medical centers | 12 (12.9) | 30 (32.7) | 4 (4.3) | 7 (7.4) | 23 (25.3) | 16 (17.2) |
| Social networks for Informing and setting and reminding of the appointment | 16 (17.2) | 12 (12.9) | 0(0) | 4 (4.3) | 20 (21.5) | 4 (4.3) |
Frequency of Use, Level of Satisfaction, and the Year of Use Starting of Each Digital Technology a
According to Table 4, the most common reason for not using "Administrative and communicative" technologies was a lack of access. For the "Digital microscope," the primary reason was expense, and for other technologies, the main reason cited was a lack of need.
| Variables | Reasons of Non-use No. (%) | ||||
|---|---|---|---|---|---|
| No Need | Expensive | Time-Consuming | Lack of Training | Inaccessibility | |
| Intraoral digital radiography | 12 (12.9) | 4 (4.3) | 0 (0) | 0 (0) | 8 (8.6) |
| 3D digital radiography (CBCT) | 22 (23.6) | 6 (6.5) | 0 (0) | 2 (2.3) | 6 (6.4) |
| Oral cameras | 45 (48.5) | 16 (17.3) | 6 (6.4) | 2 (2.1) | 10 (10.7) |
| Intraoral scanner | 37 (39.7) | 36 (38.7) | 4 (4.3) | 2 (2.1) | 10 (10.7) |
| CAD/CAM system | 29 (31.2) | 18 (19.5) | 4 (4.3) | 10 (10.8) | 22 (23.6) |
| Digital color determinate | 42 (45.1) | 6 (6.5) | 4 (4.3) | 17(18.2) | 24 (25.9) |
| Smile design software | 38 (40.8) | 6 (6.5) | 4 (4.3) | 21 (22.6) | 20 (21.5) |
| 3D printers | 38 (40.8) | 33 (35.5) | 4 (4.3) | 6(6.5) | 8 (8.6) |
| Digital microscope | 31 (33.4) | 36 (38.7) | 4 (4.3) | 2 (2.1) | 12 (12.9) |
| Information collection software and filing patients' files and managing the center | 4 (4.3) | 7 (7.4) | 18 (19.3) | 16 (17.3) | 32 (34.5) |
| Information website for scheduling appointments and reminders | 22 (23.6) | 6 (6.4) | 13 (13.9) | 16 (17.2) | 28 (30.1) |
| Communication software with other centers including radiology, Insurance, laboratories and other medical centers | 8 (8.6) | 1 (1.1) | 13 (14.2) | 0 (0) | 25 (26.2) |
| Social networks for Informing and setting and reminding of the appointment | 19 (20.4) | 0 (0) | 12 (12.9) | 0 (0) | 34 (36.7) |
Frequency of Reasons for not Using Digital Technologies by Dentists of Zahedan, Iran
5. Discussion
Digital tools and applications are now prevalent in routine dental practice. This trend toward digitization and technological developments must be integrated into dental curricula to prepare future dentists. There is a need to establish universally accepted digital education standards, at least within the dental schools of each country.
Digitalization represents a significant transformation in dental education, revolutionizing all aspects of dental care. Enhanced communication and e-learning facilities will motivate students, making learning more enjoyable and providing meaningful educational experiences that are relevant to their daily routines (5).
The present study investigated ninety-three general and specialist dentists working in private and public medical centers in Zahedan, Iran. According to the results of this study, the use of digital technologies among dentists in Zahedan was low (60.2%), moderate (35.5%), and high (4.3%).
The use of digital technologies was higher in male dentists than in female dentists. This study found a significant relationship between the use of technology and the years of experience among dentists. The lowest use of technology was observed in dentists with 5 - 10 years of experience, moderate use in those with more than 10 years, and the highest use in those with 1 - 4 years of experience. This finding aligns with the studies of Van der Zande et al. (21) and Muhlemann et al. (22), which found that younger and recently graduated dentists used more technology. Other studies have also confirmed the tendency of younger individuals to use new technology more frequently (23, 24).
This trend is explained by the hypothesis of "Digital Natives," which suggests that younger people, who have grown up with digital technology, are more inclined to use digital tools compared to "Digital Immigrants," or older people who have had to adapt to digital advancements later in life (1). However, some studies consider the effect of age on technology use to be unclear (25-27).
Another result of this study was the absence of a significant relationship between the number of digital technologies used and the level of degree (general and specialist dentists), which contrasts with the findings of Van der Zande et al. (21), where specialists used digital technologies more than general dentists. It is important to note that in the present study, the number of specialists was almost half that of general dentists. Additionally, the types of technologies examined in these two studies were not entirely the same. In this study, general dentists used more CAD/CAM systems, unlike in the study by Muehlemann et al. (22), where specialist dentists used digital microscopes more frequently.
According to the results of this study, the use of digital technologies had a significant relationship with the workplace, with moderate and high usage levels being more prevalent in private offices and clinics. This may be due to the higher costs associated with providing these technologies, which are often more financially supported in private settings.
Another finding of the study was the significant relationship between the use of digital technologies and the amount of education (not at all, somewhat, completely). Dentists with somewhat complete education had moderate to high use of digital technologies. Among those who used digital technologies, the highest amount of training was through face-to-face lectures, while the largest group of non-users had received no training.
The level of use of clinical and diagnostic technologies was higher than that of administrative and communicative technologies, which contrasts with the results of Van der zande et al. (21). In the current study, the number of clinical and diagnostic questions was nearly double that of communicative and administrative questions, potentially explaining the difference in findings.
The most commonly used administrative and communicative digital technologies among dentists were "Communication software with other centers, including radiology, insurance, laboratories, and other medical centers," followed by "Social networks for informing, setting, and reminding of appointments." These technologies began to be widely used between 2015 and 2018.
Dentists who did not use this group of technologies cited "Inaccessibility," "Unnecessary use," and "Time-consuming" as the most common reasons for non-use. One of the reasons for the greater use of "Communication programs or software with other centers" is the requirement for electronic registration of radiology and prescriptions by insurance companies in the country. In contrast, the limited use of "Information and scheduling and reminder websites" is attributed to the lack of proper internet access (including the filtration of some social media platforms in the country) and perceived unnecessity by dentists.
In the study by Muhlemann et al. (22), the use of digital technologies in dental offices was different: Ten percentage of offices used social networks, 95% used patient and office management software, 73% used appointment management software, 53% digitally registered patients' dental records, and 24% used treatment and planning software, which contrasts with the percentages found in our study.
In this study, digital radiography was the most commonly used technology among participants, similar to the findings of Van der zande et al.'s study (21), with its use mainly beginning between 2015 and 2018. The adoption of other digital clinical and diagnostic technologies started mostly after 2019.
In the present study, the usage levels of intraoral scanners, CAD/CAM systems, smile design software, and digital color determination devices were as follows: Ten people (10.6%) used intraoral scanners, 4 people (4.3%) used CAD/CAM systems, and none (0%) used digital color determination devices.
According to recent studies, CAD/CAM technologies are taught in most dental schools in North America (93%), while other digital applications have less penetration (19). Intraoral cameras have been found to increase patient satisfaction with crown treatments and are positively perceived by students, while faculty members are neutral on this technology (18).
Despite the numerous advantages of digital technologies, such as reducing the patient's time in the office, increasing work speed, eliminating the nausea reflex associated with traditional impression methods (as with intraoral scanners and smile design software), allowing treatment design without the patient's presence, and providing greater accuracy and performance (28), the use of these technologies was low in our study. The main reasons for non-use cited by dentists in Zahedan were "No need," "Inaccessibility," and "Expense," which are consistent with the reasons found in other studies (21). In the study by Muhlemann et al. (22), 23% of dental offices used CAD/CAM systems.
The study by Tran et al. (29) aligns somewhat with our study's results, showing that most respondents did not use any digital technologies.
In the current study, the highest level of dissatisfaction was related to the "Use of program and communication software with other centers," while dissatisfaction with other technologies was 0%. This contrasts with Van der zande et al.'s study (21), where the level of dissatisfaction was reported to be 31%.
Considering that studies similar to the present study have not been conducted in Iran and are minimal in other countries, the ability to examine similarities and differences in dentists' attitudes across different communities was limited. Additionally, while the design of this questionnaire was partly based on the questions from previous studies (21, 22, 29), most of the questions were self-developed, focusing on standard and current technologies relevant to dental centers worldwide and in Iran for the years 2022 - 2023. The Van der zande et al. study (21), conducted in 2015, required updates and modifications to reflect the evolving needs of dentists. Similarly, technologies introduced in recent years need to be updated and modernized, which naturally affects the level of use and satisfaction among dentists (24).
Furthermore, differences in the study's timing and location, which align with the essential needs of the dental community and even cultural differences, could contribute to variations in the results (21). Another difference lies in the sample size; the current study was conducted at the city level, whereas other studies were examined at the national level. On the other hand, the adoption of digital technologies for dental education and care has increased among dentists in dental centers in countries with advanced economies (21).
This indicates that dentists must continually update their knowledge of new technologies. With the internet serving as an excellent source of information, practitioners have a perfect opportunity to learn about newly developed technologies and incorporate them into their practice (1). Dentistry is not exempt from the growing trend of digitization and its associated benefits. However, issues such as lack of proper access, high costs, and insufficient information have limited the use of digital technologies, highlighting the need for more training in this field for dentists. It is crucial to integrate relevant topics into the educational curriculum and facilitate access to digital equipment by relevant institutions and organizations.
Given the limitations of this study's sample size, similar studies on a broader scale in other cities and provinces are recommended. Additionally, investigating the factors that limit the use of digital technologies and providing solutions to address these barriers is necessary.
5.1. Conclusions
This study investigated the frequency of digital technology use among 93 dentists in Zahedan through a comprehensive questionnaire. The findings revealed that the use of digital technologies was generally low (60.2%) and was influenced by individual factors such as gender, experience, workplace, level of education, acceptance of the necessity of use by the dentist, as well as environmental factors including access to services, costs of use, and time required.
Based on the results of this study, it is essential to provide more training for dentists and facilitate better access to digital technologies.
