1. Background
The rate of mortality in an intensive care unit (ICU) is one of the most important criteria for the evaluation of a hospital. In fact, the care given to ill patients in ICUs that are equipped with high technology equipment is the basic component of modern health care and the ultimate goal is to reduce mortality in patients. Many medical centers are trying to determine the causes that change the mortality rate in an ICU, due to the fact that this information can be categorized according to the health status and used to decrease the mortality (1).
Different levels of mortality have been reported in the literature depending on the various ICU facilities and conditions of the referred patients. The mortality rate in some reports varied from 14.5% to 44.7% (2-4). Reference of ill patients from other hospitals, admission in different work shifts, multiple trauma, and nosocomial infection are considered as risk factors for mortality (1, 5, 6).
However, most of these studies have been performed in ICUs specific for adults and there is not enough information about ICUs specifically for children. This study aimed to determine the prevalence of different causes of hospitalization and prognosis of patients admitted to the ICU of the Abuzar children’s hospital in Ahvaz, which is the main referral pediatric hospital in the south west of Iran.
2. Methods
This retrospective study was conducted in the 8-bedded pediatric ICU (PICU) of the Abuzar pediatric hospital in Ahvaz, Iran, after approval by the institutional review board. It is a tertiary PICU that is accepting patients aged 1 month to 16 years old. The data were collected retrospectively from medical records including: age, gender, vital signs, level of consciousness, diagnosis, referring center, duration of the bedridden condition, and condition at discharge. The patients were followed up during the hospital stay and the outcome measures were recorded as “died” or “survived” at the end of the hospital stay.
The study population in about one year consisted of 731 consecutive patients; 43 patients who were discharged against medical advice, and in whom the outcome was not known, were excluded. In addition, we excluded patients with less than a 3-hour duration of admission, multiple traumas, and post-surgery patients. All variables were compared using the Student’s t-test, Mann-Whitney U-test, and Chi-square test (for quantitative and qualitative variables when appropriate). In addition, the risk was expressed as odds ratio (OR) with 95% confidence interval (CI); P values < 0.05 were considered statistically significant. Children were grouped according to age. Multivariate analysis was used to evaluate the effect of gender and age on the outcome in the PICU.
3. Results
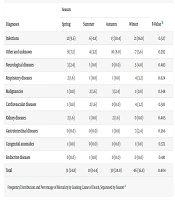
Out of the 688 included patients, 55.6% were male and the mean age was 2.7 (SD = 3.4) years. The most common age group was under 2 years (65.8%) and common causes for admission were pneumonia (22.9%), bronchiolitis (8.6%), septicemia (7.9%), and seizure disorders (6.9%). The frequency of admitted boys with poisoning, scorpion sting, and snakebite was 2 times higher than of girls; conversely, 2 times more girls than boys were admitted with diabetic ketoacidosis (DKA). Table 1 shows the causes of admission and the frequency of mortality in relation to each disease.
Table 1.
The Frequency of Admission and Mortality in Relation to the Diseasesa
| First Diagnosis | Admission (688) | All “Died” Cases (114) | Mortality for Each Diagnosis |
|---|---|---|---|
| Pneumonia | 20.5 | 21.6 | 17.4 |
| Bronchiolitis | 8.6 | 0.9 | 1.7 |
| Sepsis | 7.9 | 16.2 | 34.6 |
| Convulsion | 6.9 | 6.3 | 15.6 |
| CHD | 6.7 | 9 | 20.9 |
| Metabolic disorder | 5.2 | 4.5 | 13.9 |
| Scorpion sting | 5.1 | 0.9 | 6.2 |
| Diabetic ketoacidosis | 4.7 | 0.9 | 3.1 |
| Gastroenteritis | 4.7 | 3.6 | 12.5 |
| Asthma | 4.4 | 1.8 | 6.9 |
| Meningitis | 3.3 | 5.4 | 27.3 |
| Chronic renal failure | 3.1 | 5.4 | 28.6 |
| Liver dysfunction | 3 | 5.4 | 31.6 |
| Neurologic diseases | 2.7 | 5.4 | 21.1 |
| Poisoning | 3.8 | 0.9 | 7.7 |
| Others | 9.6 | 10.8 | - |
Abbreviation: CHD, congenital heart disease.
aValues are expressed as %.
The mean duration of hospitalization was 3.3 (SD = 3.7) days. The mortality rate was 16.5% with 2.2 (SD = 3.2) years as mean age and 51.8% of them were male. Overall, the most common causes of mortality were pneumonia (21.6%) and sepsis (16.2%); however, the mortality rate was higher in patients admitted with sepsis, liver failure, chronic renal failure, and meningitis (34.6%, 31.6%, 28.6%, and 27.3%, respectively). Furthermore, the mortality rate in patients admitted with pneumonia and bronchiolitis was 17.4% and 1.7%, respectively.
The mortality rate was significantly higher in children younger than 2 years (P = 0.044). The most common cause of admission and mortality in patients younger than 7 years was pneumonia; however, in the older group, they were non-infectious diseases (Table 2).
Table 2.
Mortality in Each Age-Groupsa
| Age Groups, y | Mortality | Mortality Rate in Each Age Group | Admission |
|---|---|---|---|
| < 2 | 74.3 | 18.6 | 66.1 |
| 2 - 7 | 19.5 | 14.2 | 22.7 |
| > 7 | 6.2 | 9.2 | 11.2 |
aValues are expressed as %.
About 53% of patients were referred from near and far neighbor towns (under 100 and 200 kilometer, respectively), however, the mortality rate was not significantly different (P > 0.05).
On arrival in the ICU, 7.1% of patients were intubated and among the ultimately dead children, 24.6% were initially intubated [P < 0.001, OR = 8.63 (95% CI, 4.69 - 15.8)]; on the other hand, 8.3% of admitted patients had a decreased level of consciousness and among the ultimately dead children, 17% suffered from a pre-admission decreased level of consciousness [P = 0.015, OR = 0.38 (95% CI, 0.17 - 0.85)]. In addition, the mortality rate in initially intubated patients and in those who suffered from a decreased level of consciousness was 57.1% and 20.5%, respectively (Table 3).
Table 3.
Factors Affecting Outcome of Children Admitted to the PICUa
| Variable | Survivors (n = 574) | Non-Survivors (n = 114) | P Value |
|---|---|---|---|
| Age, y | 2.79 ± 3.46 | 2.21 ± 3.22 | 0.1 |
| Age group (younger than 2 y) | 66.1 | 74.3 | 0.044b |
| Sex (male) | 57.6 | 51.8 | 0.24 |
| Intubated patients | 3.6 | 24.6 | < 0.001b |
| Decreased level of consciousness | 7.3 | 17 | < 0.001b |
| Fever | 10.7 | 9.2 | 0.63 |
| Tachypnea | 43.5 | 48.8 | 0.86 |
| Referral site | 0.15 | ||
| In town | 48.6 | 41.2 | |
| Neighbor towns | 51.4 | 51.8 |
aValues are expressed as mean ± SD or %.
bStatistically significant difference.
Tachypnea was seen in 43.7% and fever (central body temperature above 38°C) was seen in 10.3%, however, these parameters had no significant correlation with the mortality rate (P > 0.05).
A total of 65% of patients were transferred from emergency departments to the ICU and 18% from the general ward; however, the mortality in patients referred from the emergency department was significantly higher (18.7%, P = 0.034).
The rate of hospitalized patients in the morning shift (from 8 AM to 2 PM) was 16.7%; it was 36.2% in the afternoon shift (2 PM to 8 PM), and 47% in the long night shift (8 PM to 8 AM) (P > 0.05). The mortality rate in the morning, afternoon, and in the first 6 hours and second 6 hours of the night shift was 32.4%, 24.3%, 27.1%, and 16.2 %, respectively (P = 0.008).
The average duration of stay in the ICU in the “died” group was 4.1 (SD = 5.3) days while it was 3.1 (SD = 3.2) days in ameliorated patients (P = 0.017); furthermore, the mortality rate was higher in patients staying less than 1 day and more than a week (P < 0.001, OR = 2.49 (95% CI, 1.36 - 4.55).
The multiple linear regression analysis showed that the younger than 2 year old patients, decreased level of consciousness, pre-admission intubated patients, and prolonged stay in PICU were significantly correlated with the mortality (P = 0.005, R = 0.178).
4. Discussion
The aim of this study was to identify the main causes of hospitalization and mortality in the PICU of the Abuzar pediatric hospital. According to our study, pneumonia and severe infections were the most common causes of PICU admission and mortality. Seizures, decreased level of consciousness, electrolyte abnormalities, and instability of vital signs were the other common conditions for admission.
The mortality rate in this center (16.5%) is comparable with the study by Morales (2) in America (14.5%), Bellad (3) in India (16.7%) and the study by Chen (6) in Taiwan (22%), however, it is less than in the study by Coplan (4) in Turkey (44.7%) and Abrishamkar (7) in Iran (37.4%). This can be due to developing PICU equipment in recent years and the lack of trauma patients and other patients who required surgery in our patients group.
The most common age for hospitalization and death was younger than 2 years and in this age group, pneumonia, and septicemia were the most common causes of death; however, respiratory problems are the most common cause of death in most of ICUs now (6-10). Although pneumonia was the most common cause of mortality, the incidence of death in patients referred with septicemia, liver failure, chronic renal failure, and meningitis was significantly higher than other diseases.
In some studies, reference of patients from faraway cities and transfer of patients from other hospitals are considered as risk factors for increased mortality (5, 11, 12); however, no significant association was observed in our study and in some other studies (5, 13-15).
Intubated patients and reduced level of consciousness on arrival at the ICU are 2 significant risk factors for mortality and therefore, it is necessary to pay attention to the transfer of these patients to prevent further hypoxemia and other complications of uncontrolled ventilation, such as pneumothorax formation.
In some studies, the mortality rate of patients was significantly associated with the work shifts of the hospital personnel (6), which was not confirmed in some other studies (2). In our study, the lowest mortality was observed between 2 AM and 8 AM (second part of the night shift) and the highest between 8 AM and 2 PM (morning shift). This difference was statistically significant and it might be due to the change in ICU physicians and nurses (who are more familiar with the patient’s problem) and the higher number of doctor’s orders and medical procedures in the morning shift. Furthermore, mortality was significantly associated with the duration of the stay in the ICU. Most deaths occurred in patients who stayed for less than 1 day and more than 7 days, which can be related to the higher frequency of mortality in severely ill patients and in patients with chronic diseases such as chronic renal and liver failure. This finding is similar to the study by Hui that showed a higher mortality rate in prolonged stays in the ICU (16). However, some studies reported that most deaths occurred in the first 4 days of ICU admission (2, 6, 7).
In our study, the prevalence of hospitalization and mortality was not significantly different in boys and girls in most cases. The higher incidence of poisoning, scorpion sting, and snakebite in boys and the higher prevalence of DKA in girls need to be further investigated.
In conclusion, higher mortality in very young children, especially due to severe infections, indicates that we need better equipment for the treatment of patients of this age (including more compatible ventilators and treatment protocols). Furthermore, PICU established with well-trained personnel in every pediatric ward, prevents the need for referring intubated patients and possibly would reduce the mortality.