



1. Background
Infertility is a common problem that affects women and men worldwide, as about 10-15% of couples are infertile. The rate of infertility has increased by 50% over the past two decades. According to the World Health Organization (WHO), between 8% and 12% of all couples in the world experience some kind of infertility during their reproduction period. This means that 50 to 80 million people worldwide are infertile or sub-fertile (1). In Iran, a large study was performed in 2008 on 12,285 couples in 30 provinces indicated that the prevalence of infertility was 8% (2). Another study in Iran showed the prevalence of infertility was 2.5% in 2001, and this national study estimated the prevalence of primary infertility at 1.6% (3). In a study, primary infertility and secondary infertility were estimated at 1.7% and 10.5%, respectively (4). Nowadays, many infertile couples (40 - 50%) can be pregnant with the advent of science and the use of modern methods of infertility treatment (5).
One of the treatment methods for infertile women is the use of ovulation induction, and new treatments, commonly as ART, have raised hopes for many infertile couples. Ovulation induction is the most common method of treating infertility in which ovaries are stimulated to produce multiple follicles (6). Ovulation induction is a widespread method for treating infertility not only for women with ovarian disorders such as amenorrhea or ovulation but also for infertile couples with blocked fallopian tubes, low sperm count, defective sperm, unexplained infertility, and other factors (7, 8).
About 30 - 40% of infertility in women is due to tube and peritoneal factors. Diagnostic methods such as hysterosalpingography, laparoscopy, hysterosalpingography, and hysteroscopy are used to diagnose these factors, and the type of treatment will be determined based on the diagnosis. Hysterosalpingography uses a real-time form of X-ray called fluoroscopy to examine the uterus and fallopian tubes. It is performed in the early stage of the menstrual period (6th-12th day of menstrual period) and usually is done in radiology clinics (9). In addition to diagnostic applications, hysterosalpingography has a therapeutic effect on the success of fertility so that during hysterosalpingography, many subtle adhesions and spasms of uterine tubes are resolved after the injection of contrast material; this increases the spontaneous pregnancy rate and the efficacy of ovulation induction medications (10).
2. Objectives
Considering the lack of similar studies for the investigating of the effect of hysterosalpingography on the success of pregnancy in our country, the present study was designed to determine the therapeutic effects of this diagnostic method on the success of pregnancy in women with a history of primary or secondary infertility.
3. Methods
A descriptive-analytical study was done in 2016 under ethical code IR.ZAUMS.REC.1395.55. The study population in this study included women with primary or secondary infertility who referred to the Gynecology and Radiologic Clinic of Ali-ibn Abitalib Hospital from February to Aguste 2016. The minimum sample size was 100. The inclusion criteria for the study included a definitive diagnosis of infertility and informed consent for participation in research. The exclusion criteria included any abnormalities of the uterus, hydrosalpinx, not flushing of the contrast material, and the absence of the uterine (obstruction of the internal or external os of the cervix).
In the present study, data were gathered in 12 items, including the results of HSG, the outcome of pregnancy, and the type of pregnancy (spontaneous or induced). After confirming the validity and reliability of data collection tools and obtaining informed consent, the researcher selected the participants using a convenience sampling method.
After performing the examinations, initial tests, and procedures, as well as the R/O of acute pelvic infection disease by expert gynecologists, the patient was referred to a radiologist for HSG. All patients in this study underwent HSG, including those who received ovulation induction and those who did not receive any special treatment for infertility. Data were analyzed by SPSS version 21 software after collection and coding. Descriptive statistics such as frequency, mean, standard deviation, minimum, and maximum were used for quantitative variables, and the Levene test was used for the equality of variances. The chi-square tests, Fisher exact test, and independent T-test were used to determine the relationship between variables. The significance level of the test was considered to be 0.05.
4. Results
The findings of this study showed that the mean age of the participants in the study was 30.36 years (± 5.25), and the mean infertility duration was 4.81 years (± 2.81). Most of the participants in the study (75%) had primary infertility, without surgery history (71%), without obstruction (89%), and with a treatment history for infertility (60%). None of the patients had adhesion, abnormal uterus, and hydrosalpinx. In the HSG report, most of the participants (83%) were normal, and the minority (6%) had adhesion (Table 1).
| Variable | Mean ± SD | Min | Max | No. (%) |
|---|---|---|---|---|
| Age (y) | 30.36 ± 5.52 | 19 | 44 | |
| Infertility duration (y) | 4.81 ± 2.81 | 1 | 13 | |
| Infertility | ||||
| Primary | 75 (75) | |||
| Secondary | 25 (25) | |||
| Surgery history | ||||
| + | 29 (29) | |||
| - | 71 (71) | |||
| Obstruction | ||||
| + | 11 (11) | |||
| - | 89 (89) | |||
| Treatment | ||||
| + | 60 (60) | |||
| - | 40 (40) | |||
| Results of HSG | ||||
| Normal | 83 (83) | |||
| Obstruction | 11 (11) | |||
| Adhesion | 6 (6) |
Demographic Variables of the Participants in the Study
The results of this study showed that 20 (20%) participants in the present study get pregnant after the study, including 11 (27.5%) spontaneously and 9 (15%) by ovulation induction. The chi-square test showed no statistically significant relationship between the type of pregnancy and the outcome of pregnancy (P = 0.126) (Table 2).
| Pregnancy Outcome | Treatment Type | Test Results | |
|---|---|---|---|
| Ovulation Induction, No. (%) | Spontaneous Pregnancy, No. (%) | ||
| + | 9 (15) | 11 (27.5) | P = 0.126, χ2 = 2.344 |
| - | 51 (85) | 29 (72.5) | |
| Total | 60 (100) | 40 (100) | |
Absolute and Relative Frequency of Pregnancy Success Through Ovulation Induction and Spontaneous Pregnancy
The results of this study showed no significant relationship between the age and history of abdominal surgery and HSG in both groups of women with spontaneous pregnancy and ovulation induction. Also, the results of the study showed that the mean duration of infertility was lower in spontaneously pregnant women than those who were not pregnant. The independent t-test indicated a statistically significant relationship between the mean duration of participants' infertility and the success of spontaneous pregnancy. The findings also indicated that the mean duration of infertility in pregnant women following ovulation induction was lower than that in those who were not pregnant, but there was a statistically significant relationship between the mean duration of infertility and the success of pregnancy with ovulation induction (Table 3).
| Duration of Infertility (Years) | Outcome of Pregnancy | T-test | P Value | |
|---|---|---|---|---|
| Positive, Mean ± SD | Negative, Mean ± SD | |||
| Pregnancy type | ||||
| Spontaneous pregnancy | 2.68 ± 2.88 | 4.94 ± 2.33 | -2.567 | 0.014 |
| Ovulation Induction | 4.83 ± 4.19 | 5.19 ± 2.63 | -0.346 | 0.731 |
Relationship Between the Duration of Infertility and the Success of Spontaneous Pregnancy and Ovulation Induction in the Investigated Sample
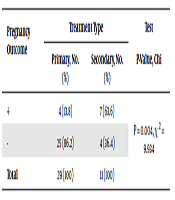
Also, Fisher's exact test showed a statistically significant relationship between the frequency of an infertility type and the success rate of spontaneous pregnancy (P-value = 0.004) (Table 4).
| Pregnancy Outcome | Treatment Type | Test Results (P-Value, Chi) | |
|---|---|---|---|
| Primary, No. (%) | Secondary, No. (%) | ||
| + | 4 (13.8) | 7 (63.6) | P = 0.004, χ 2 = 9.934 |
| - | 25 (86.2) | 4 (36.4) | |
| Total | 29 (100) | 11 (100) | |
Relationship Between Type of Infertility and Spontaneous Pregnancy Success in Patients
5. Discussion
The results of the study showed a relative success in women's infertility treatment. The results of several studies on the therapeutic effects of HSG indicate a high variation of 18 - 75% in the success of pregnancy (11).
Mackey et al. (1971), in their study, reported pregnancy after six weeks in 30-50% of the patients following normal HSG (12). Generally, the success rate of pregnancy after HSG was attributed to three factors of infertility period before HSG, frequency of intercourse after HSG, and the presence/absence of concomitant treatment with HSG (11). Other factors, including the volume and type of solution, play an important role in the likelihood of success. Studies have shown that using fat-based solutions has a higher ability to open the fallopian tubes (12). Some studies have shown that the success rate of pregnancy after HSG differs in different treatment centers and populations. In other words, the role of environmental factors and polymorphism is decisive (13, 14).
The results showed that the success rate of pregnancy was higher in patients with HSG who did not use ovulation induction methods than in the group using induction ovulation methods. It would definitely be said that HSG has far more effects on the success of pregnancy than had ovulation induction. Ming-Hueilin et al. (2013), in their study to assess the treatment of infertile women due to unilateral fallopian obstruction with ovulation induction and IUI, stated that complementary therapies, such as IUI and ovulation induction with HSG have different pregnancy outcomes depending on various factors such as occlusion location (proximal, medial, and distal) and the severity of obstruction (unilateral, bilateral) (15).
Yi et al. (2012) stated that induction ovulation with HSG could be used as an initial treatment. The success rate of pregnancy is affected by the type of blockage. They stated that women with proximal tubular obstruction had better results than those with distal obstruction (16). Perhaps, the reason for the lower birth rate in women with ovulation induction than in women with spontaneous pregnancy was the difference in their tubal problems. Another important factor in the prevalence and incidence of infertility is the physical condition and body mass (BMI). Mothers with a low BMI, in addition to thinner tubes, suffer from a lack of sex hormones and infertility due to the low-fat content required for the anabolism of sex hormones. There was no statistically significant relationship between the age of patients, the type of blockage, and the outcome of pregnancy.
Ming-Hueilin et al. (2013) also found no significant association between the patient's age and the pregnancy rate after HSG (17). Age is known to be an effective factor in the success of pregnancy in many studies. It is scientifically and experimentally expected that the success of pregnancy is much higher in younger women. (18, 19). The results showed no statistically significant relationship between the success rate of spontaneous pregnancy and ovulation induction and the history of abdominal surgery. Honoré et al., in 1999, showed a high success rate of spontaneous pregnancy in women undergoing bilateral microsurgery in fallopian tubes compared to women who used the transcervical technique to open the blockage of the fallopian tube, but this difference was not significant. On the other hand, in women with unilateral microsurgery, there was no significant difference in the prevalence of pregnancy success (17). In
A study by Jacob et al. (2006), the results of their study showed that the history of abdominal surgery in infertile women due to tubal factor was almost twice women with unexplained infertility. It, therefore, seems that the history of abdominal surgery causes infertility through the obstruction of fallopian tubes more than do other related factors. It can be said that in women with a history of abdominal surgery due to adhesions, the probability of pregnancy success, spontaneously, or under the influence of HSG, would be lower (20).
The results showed a statistically significant relationship between the mean duration of infertility of patients and the infertility type and the success of pregnancy in women with spontaneous pregnancy. Women with a short duration of infertility and secondary infertility are more likely to become pregnant. Dessolle et al. showed a significant relationship between the duration of infertility and the type of infertility and pregnancy outcomes. They stated that a long duration of infertility would reduce the probability of pregnancy (21). Stamatellos et al. did not find a significant relationship between the type of infertility and pregnancy outcomes in women with polyps. This inaccuracy may be due to the presence of polyp lesions in the patients (22-24).
In conclusion, the results of this study showed that the use of HSG as a therapeutic method in the presence or absence of ovulation induction methods had no significant effect on pregnancy outcomes. There was only a statistically significant relationship between the duration of infertility and pregnancy outcome in spontaneous pregnancy, but none of the variables under study had any relationship with pregnancy outcomes. Hence, it can be said that using hysterosalpingography as a therapeutic approach is not effective, but HSG can have therapeutic effects in women with early infertility.
