1. Background
Candida species are endogenous or exogenous opportunistic pathogens in the hospital setting. Endogenous Candida colonizes the mucosa and becomes invasive towards a systemic infection in predisposed patients. Exogenous Candida species may enter the body through medical devices or the hands of health care workers (1). Opportunistic yeast infections are mostly due to Candida and reflect an increasing problem in pediatric hospitals, now being a major cause of morbidity and mortality in hospitalized children and the second-most common causes of sepsis (2). Pediatric patients mainly at risk for developing invasive candidiasis are low-weight or preterm neonates and children admitted to ICUs, children with acquired or congenital immune deficiency, children with underlying malignancy, and children treated with corticosteroids (1, 3, 4). In pediatric patients, candidemia is associated with prolonged hospitalization and increased costs with a reported attributable mortality rate of 20% - 30% (4). Being clinically similar to sepsis caused by bacteria, candidemia is not associated with any specific signs and symptoms (4). C. albicans is still the main cause of nosocomial fungal infections; however, non-albicans Candida species are increasingly being reported, which species may have lower susceptibility to antifungal agents. For example, C. parapsilosis is accounting for 10% - 20% of the episodes of candidemia among neonates and children. It is reported that nearly 20% of isolates belong to this species are resistant to amphotericin B, which is one of the most commonly used antifungal agents (5). C. krusei and C. glabrata are two species that are resistant to fluconazole; thus prophylaxis using azoles may induce the emergence of infection with these species (6).
Patients admitted to ICU or patients with serious underlying conditions such as cystic fibrosis and cancers are frequently colonized with Candida species (7). Colonization with Candida species is a risk factor for invasive candidiasis, as it may precede serious infections in critically ill patients (8). It has been shown that patients with severe Candida infections had a previous colonization with Candida (4, 8, 9). Since the clinical manifestations of invasive candidiasis is un-specific and diagnosis of infection is lengthy and insensitive, monitoring of yeast colonization might be useful for early prophylaxis of at risk predisposed patients. In general, awareness about local epidemiology and species distribution of Candida species in hospitalized populations as well as knowledge about prior colonization can help clinicians, microbiologists and clinical epidemiologists prevent or manage suspected invasive infections or ongoing outbreaks.
2. Objectives
The main aim of this study was to obtain knowledge on Candida flora in children and the distribution of different Candida species in patients referred to children’s medical center in Tehran. Data on the microbial epidemiology of colonization is critical to finding the source of contamination and subsequent infection. Such data can help us to find out which patients will be affected and who are at risk for developing disease. Early recognition of probable nosocomial Candida infections can improve the outcome and minimize the morbidity and mortality of the related diseases. Being aware of risk factors could help neonatologists and pediatricians to instigate appropriate antifungal prophylaxis, which appears to be markedly effective in reducing the incidence of Candida colonization and invasive infections in the children’s wards. To our knowledge, this is the first study identifying Candida species isolated from pediatric patients in Iran.
3. Methods
In this descriptive cross-sectional study, yeast strains were collected between June 2014 to June 2016 from 341 pediatric patients in children’s medical center, Tehran, Iran. Yeasts were isolated from children aged 1 day to 15 years old (Table 1) via various clinical specimens including urine, stool, throat swabs, sputum, tracheal aspirates, wound discharges, dialysis fluids, and catheters. Only one sample from each patient was included. As part of routine diagnostic and therapeutic management, the clinical specimens were cultured on blood agar, chocolate agar, and MacConkey agar plates (all from Merck, Germany). The plates were incubated at 35°C and examined daily for growth for five days before considering it negative. Yeast colonies were subcultured on Sabouraud glucose agar (Difco, Detroit, MI, USA) with 0.05% chloramphenicol and 0.05% gentamycin to avoid bacterial growth, and incubated in 30°C for at least 48 hours, followed by subculturing on CHROMagar (CHROMagar Paris, France) to ensure the purity of the isolates and for preliminary species identification. CHROMagar plates were incubated at 35°C for 48 hours and evaluated for specific colony colors (10).
Table 1. Distribution of C. albicans And Non-albicans Candida Species Among Different Age Groups of Tested Children
| Age | 1 - 28 Day | 1 - 12 Month | 13 - 24 Month | 2 - 5 Year | 6 - 10 Year | 11 - 15 Year | Total | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Specimen | CA | NAC | M | CA | NAC | M | CA | NAC | M | CA | NAC | M | CA | NAC | M | CA | NAC | M | CA | NAC |
| Urine | 25 | 10 | 1 | 72 | 25 | 1 | 6 | 4 | - | 15 | 4 | - | 7 | 2 | - | 8 | 3 | - | 135 | 50 |
| Stool | - | - | - | 19 | 10 | 3 | 3 | 1 | - | 7 | 2 | - | 3 | 1 | - | 2 | 2 | - | 37 | 19 |
| Throat | 1 | - | - | 18 | 4 | - | 4 | - | - | 8 | 1 | - | 13 | 1 | - | 5 | 2 | - | 49 | 8 |
| Urine Catheter | 1 | - | - | 1 | - | - | - | - | - | - | - | - | - | - | - | - | - | - | 2 | - |
| Sputum | - | - | - | - | - | - | - | - | - | 1 | - | - | 9 | - | - | 3 | - | - | 13 | - |
| Dialysis fluid | - | - | - | 1 | - | 1 | - | - | - | 2 | - | - | - | - | - | 1 | - | - | 5 | 1 |
| Wound discharge | 1 | - | - | 6 | - | - | - | - | - | 1 | - | - | - | - | - | - | - | - | 8 | - |
| Tracheal tube | 2 | - | - | 5 | - | - | - | - | - | - | - | - | 2 | 1 | - | - | - | - | 9 | 1 |
| Mouth | - | - | - | 1 | - | - | - | - | - | - | - | 1 | 2 | - | ||||||
| Suprapubic | 1 | 1 | - | - | - | - | - | 1 | 1 | |||||||||||
| Nephrostomy | - | - | - | 2 | - | - | - | - | - | - | 1 | - | - | - | - | - | - | - | 2 | 1 |
| Eye discharge | 1 | 1 | - | 1 | - | - | - | - | - | - | - | - | - | - | - | - | - | 2 | 1 | |
| Total | 32 | 12 | 1 | 126 | 39 | 5 | 13 | 5 | - | 34 | 8 | - | 34 | 5 | - | 20 | 7 | - | 266 | 81 |
Abbreviations: CA, Candida albicans; NAC, Non- albicans Candida; M, Mix.
For precise species identification of the isolates, genomic DNA was extracted by adding a loopful of fresh colonies to 200 µL distilled water in a 1.5-mL tube; the mixture was boiled for 10 minutes, centrifuged for 2 minutes at 5000 rpm, and then the supernatant was transferred to a fresh tube and stored at -20°C until used for PCR (11).
Molecular identification of common Candida species was carried out according to an already described PCR-restriction fragment length polymorphism (RFLP) method (12). Briefly, the ITS1-5.8S rDNA-ITS2 region was amplified using a PCR mixture containing 12.5 µL of 2 × premix (Ampliqon, Denmark), 10 pmol of each ITS1 (5’-TCC GTA GGT GAA CCT GCG G-3’) and ITS4 (5’-TCC TCC GCT TAT TGA TAT GC-3’) primers (13), 3 µL of extracted DNA, and enough double-distilled water to obtain a final reaction volume of 25 µL. Conditions for PCR amplification were as follows: initial denaturation at 94°C for 5 minutes, 35 cycles of denaturation at 94°C for 30 seconds, annealing at 55°C for 45 seconds, and extension at 72°C for 1 min; and a final extension step at 72°C for 7 minutes. To achieve species discriminatory patterns, a 5-µL aliquot of each PCR product was digested with 5 U of the restriction enzyme MspI (Fermentas, Vilnius, Lithuania), 1.5 μL of relevant buffer and enough water to obtain a final reaction volume of 15 µL and incubated the mixture at 37°C for 2 hours in a PCR thermocycler.
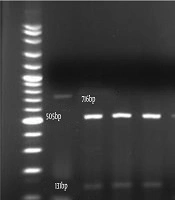
Five microliters of each PCR amplicon or 10 μL of each RFLP product was subjected to 1.5% and 2% agarose gel electrophoresis, respectively. Enzymatic digestion of PCR products yielding specific size patterns allowed us to identify each Candida isolate by comparing the patterns with PCR-RFLP profiles already described for differentiation of yeast pathogens (14) (Figure 1).

Figure 1.
Example of Agarose Gel Electrophoresis of PCR-RFLP Products of Candida Strains Isolated From Patients in Children Medical Center. Lanes 1 to16 Are C. glabrata, C. tropicalis, C. tropicalis, C. lusitaniae, C. albicans, C. parapsilosis, C. guilliermondii, C. albicans, C. parapsilosis, C. tropicalis, C. albicans, C. albicans, C. tropicalis, C. lusitaniae, C. parapsilosis, C. lusitaniae, Respectively, Lane M Is 100 Bp Molecular Size Marker
4. Results
A total of 347 yeast strains were isolated from 341 inpatients (n = 264, 77.4%) and outpatients (n = 77, 22.6%). Six clinical samples including two urines, three stool, and one dialysis fluid contained mixed Candida species. The patient group consisted of 213 males (62.5%) and 128 females (37.5%) aged 1 day up to < 15 years. Most cases were in the 1 - 12-month age group (n = 170, 49.9%) and the 1 – 28-day group (n = 45, 13.2%). The predominant Candida species isolated in this study was C. albicans (n = 266, 77%). The non-albicans Candida species accounting for 23% of the remaining isolates were as follows: C. tropicalis (n = 29, 8.4%), C. parapsilosis (n = 26, 7.5%), C. glabrata (n = 8, 2.3%), C.kefyr (n = 6, 1.7%), C. krusei (n = 4, 1.1%), C. lusitaniae (n = 2, 0.6%), C. guilliermondii (n = 1, 0.3%), C. albicans + C. parapsilosis (n = 5, 1.4%), and C. albicans + C. glabrata (n = 1, 0.3%). Most samples were obtained from general wards (n = 154) and from outpatients referred to the emergency ward (n = 77). General wards included the nephrology ward with 24 (7%) isolates, emergency room (EMR) (n = 22, 6.5%), infectious disease (n = 21, 6.2%), cardiology (n = 19, 5.6%), gastroenterology (n = 17, 5.4%), urology (n = 15, 4.4%), neonates (n = 12, 3.5%), rheumatology (n = 9, 2.6%), neurology (n = 8, 2.3%) and oncology (n = 6, 1.8%) wards. PICU, NICU, and surgery wards (n = 65 (19.1%), n = 31 (9.1%), and n = 14 (4.1%), respectively) were placed in the next ranks (Table 2).
Table 2. Distribution of C. alnicans and Non-albicans Candida Species Among Different Pediatric Wards
| Ward | NICU | PICU | General | Surgery | Outpatients | Total | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Specimen | CA | NAC | M | CA | NAC | M | CA | NAC | M | CA | NAC | M | CA | NAC | M | CA | NAC |
| Urine | 16 | 7 | - | 29 | 15 | - | 64 | 18 | 1 | 7 | 2 | 1 | 17 | 6 | - | 135 | 50 |
| Stool | - | - | - | 3 | - | 1 | 16 | 10 | 1 | 2 | - | - | 13 | 6 | 1 | 37 | 19 |
| Throat | - | - | - | 2 | 1 | - | 21 | 6 | - | - | - | - | 26 | 1 | - | 49 | 8 |
| Urine catheter | 1 | - | - | - | - | - | 1 | - | - | - | - | - | - | - | - | 2 | - |
| Sputum | - | - | - | - | - | - | 9 | - | - | - | - | - | 4 | - | - | 13 | - |
| dialysis fluid | - | - | - | 4 | - | 1 | - | - | - | - | - | - | - | - | - | 5 | 1 |
| Wound discharge | 1 | - | - | 1 | - | - | 4 | - | - | 1 | - | - | 1 | - | - | 8 | - |
| Tracheal tube | 2 | - | - | 7 | 1 | - | - | - | - | - | - | - | - | - | - | 9 | 1 |
| Mouth | - | - | - | - | - | - | - | - | - | - | - | - | 2 | - | - | 2 | - |
| Suprapubic | - | 1 | - | - | - | - | 1 | - | - | - | - | - | - | - | - | 1 | 1 |
| Nephrostomy | - | - | - | - | - | - | 1 | 1 | - | 1 | - | - | - | - | - | 2 | 1 |
| Eye discharge | 2 | 1 | - | - | - | - | - | - | - | - | - | - | - | - | - | 2 | 1 |
| Total | 22 | 9 | - | 46 | 17 | 2 | 117 | 35 | 2 | 11 | 2 | 1 | 63 | 13 | 1 | 266 | 81 |
Abbreviations: CA, Candida albicans; NAC, Non-albicans Candida; M, Mix.
The majority of clinical specimens from which Candida was isolated included specimens of urine (n = 182, 53.4%), throat swabs (n = 57, 16.7%), and stool (n = 53, 15.5%). C. albicans was the predominant species across all types of specimens. Among 29 C. tropicalis, 16 cases were isolated from the 1 - 12-month age group patients of whom 9 were bedridden in PICU; all the samples were urine samples. As compared with other species, C. parapsilosis was the second-most common species isolated from NICU. C. glabrata and C. krusei were isolated from stool, urine, and throat swabs from patients in general wards and outpatients. Six samples were mixed: Five contained mixed C. albicans and C. parapsilosis isolated from urine, stool, and dialysis fluid (n = 2, 2, and 1, respectively), and 1 contained a mixture of C. albicans and C. glabrata isolated from stool from a 1-year-old patient in the urology ward.
5. Discussion
In the present study, C. albicans was the species most frequently isolated, detected in 77% of the patients with Candida. This finding is in contrast with many other studies, in which non-albicans Candida species were responsible for approximately half of the cases (1-3, 15, 16). Surprisingly, unlike other researchers who reported C. parapsilosis as the most common non-albicans Candida species encountered in pediatric patients (1, 2, 15, 16), C. tropicalis was the second-most common species (8.5%) identified in present study, hence resembling the distribution pattern observed in adult patients. In a study by Arslankoylu et al. (17) C. albicans was the most common Candida species in pediatric patients, as well the most common species among the asymptomatic patients in the PICU. A mortality rate of 71% in patients with C. tropicalis has been reported (17). Overall, these two species have been suggested as a common cause of mortality in pediatric patients. C. tropicalis can rapidly progress from colonization to invasion (18). Fungemia with this organism appears to be more persistent, leading to longer ICU stays, and associated with higher mortality than other Candida species (18).
C. parapsilosis was the third-most common Candida species isolated in this study, with about 70% being isolated from urine samples; 30% were isolated from NICU patients, who are at the highest risk of developing candidemia. Nosocomial Candida infections may originate from endogenous strains or exogenous sources transmitted to patients via contaminated infusions, biomedical devices, or even by the hands of the health care workers. Unlike C. albicans and other Candida species, C. parapsilosis can access the blood stream and cause candidemia without prior colonization of other sites of body, by horizontal transmission from patient to patient, health care workers to patients, and medical materials to patients (5). Some outbreaks of C. parapsilosis in ICUs have been associated to cutaneous routes of transmission (5). C. parapsilosis is the second-most commonly isolated Candida species from normally sterile body sites of hospitalized patients and has been isolated from approximately one-third of neonates with gastrointestinal colonization by Candida species and from oropharynges of 23% of healthy neonates (18). Colonization of the gastrointestinal tract with C. parapsilosis occurs at a higher rate in neonates, leading to a further increased risk of candidemia (19, 20).
Previous exposure to fluconazole is associated with infection due to C. glabrata and C. krusei (5). Fortunately, a relatively low frequency of these two species was observed in this study. In addition, age more than 2 years, recent surgery, and recent exposure to fluconazole have been identified as independent risk factors for C. glabrata and C. krusei infections. While C. glabrata is the second most common species isolated in adults, it is very infrequent in the pediatric setting (1-4).
Other species such as C. kefyr, C. lusitaniae, and C. guilliermondii were rarely detected in our study. Nevertheless, an outbreak caused by C. guilliermondii was reported in Brazil (21), however, this species was very common in Honduras (15). These emerging pathogens, have shown some degree of primary resistance to azoles and amphotericin B and may have worse clinical outcomes, particularly so for C. lusitaniae, which might be less susceptible to amphotericin B therapy (6). C. guilliermondii is a rare and uncommon species associated with fungemia in patients with cancer or hematological neoplasia as a result of central venous catheter usage, with a high mortality rate (22). However, in a retrospective study, Arendrup et al. concluded that although collectively non-albicans Candida species accounted for the majority (56%) of infections, there was no discernible difference between C. albicans and non-albicans Candida species in terms of demographics, underlying disease, clinical features, dissemination, and mortality (23).
Although in this study most Candida isolates were recovered from general wards, the number of isolates recovered from PICU and NICU were also significant. Likewise, Peman et al. illustrated that a higher rate (67.9%) of fungemia episodes occurred in patients admitted to general pediatric or surgical wards (24).
There is an association between adherence capacity of the organism, its ability to colonize human epithelial cells and progression to disease (18). Most likely, the initial step in fungal pathogenesis is colonization. Endogenous Candida within the gastrointestinal tract establish colonization which is recognized as an independent risk factor for invasive mycosis and an increased morbidity and mortality in ICU patients (1, 3). ICU patients are frequently colonized with different Candida species, and it has been reported that colonization with Candida species occurs in approximately 70% of pediatric patients in the PICU; in one study about 90% of the patients who developed candidemia were colonized, 75% with the same Candida species (9). Presence of central venous catheter was also an independent risk factor for colonization (3).
Colonization is defined as the isolation of Candida species from at least one surveillance site. In our study, most Candida species were isolated from urine samples at all the wards. The presence of yeast in the urine may be a sign of infection, colonization, or contamination.
Candiduria occurring in critically ill patients should initially be regarded as a marker for the possibility of invasive candidiasis. The first step in evaluation is to verify funguria by repeating the urinalysis and urine culture (25). Urinary catheterization and broad-spectrum antibiotic usage are the most common risk factors for symptomatic candidiasis in pediatric patients (17). According to Sobel et al., candiduria in the critically ill newborn very often reflect candidemia or disseminated candidiasis and may be accompanied by obstructing urinary tract fungus ball formation (26). All common Candida species are capable of causing urinary tract infections (UTI). It appears that C. glabrata and C. tropicalis are better adopted to the urinary tract environment. With increasing use of azole prophylaxis, these fluconazole-resistant Candida isolates may not only be well adapted to the kidney and collecting system but also more difficult to eradicate than C. albicans (27). However, in many studies C. albicans is still the most common cause of UTIs in children. De Sousa reported a higher prevalence (45%) of C. albicans in urine samples of outpatients (28).
A total of 23.5% of our Candida strains were isolated from upper respiratory tract samples including throat, sputum, and tracheal tube samples. Generally, Candida pneumonia is a rare condition, and the effect of Candida colonization of the respiratory tract on candidemia and on mortality and morbidity is unclear. However, in a study it was found that Candida respiratory tract colonization is associated with increased hospital mortality and prolonged hospitalization (7). The presence of Candida in endotracheal secretions needs to be interpreted in a clinical context (7), as Candida species are frequent asymptomatic colonizers of the upper respiratory tract, especially in hospitalized patients (9). In a primary Candida pneumonia, concomitant Candida esophagitis and colonization of the upper respiratory tract is frequently seen (7). Frequent use of antibiotics, oral and inhaled steroids predispose cystic fibrosis (CF) patients to oral colonization by Candida species as evidenced in a study in which C. albicans was isolated from the respiratory tract in 93% of CF patients (7, 29). Singhi et al. showed that colonization by Candida species occurred in 45 (69%) of patients admitted to PICU, with oropharyngeal (52%) and rectal (43%) colonization predominating; the colonizing species were C. tropicalis (34.2%), C. parapsilosis (28.8%), and C. albicans (14.4%) (9). Endogenous flora in the GI tract has been known to be an important local defense mechanism that prevents fungal proliferation (3). In patients with neoplastic disease, mucosal disruption caused by cytotoxic chemotherapy and abrogation of the normal gastrointestinal flora by antimicrobial therapy, create a permissive environment that allows Candida to invade the mesenteric circulation (1). In our study, 56 isolates of Candida were isolated from stool samples that it could be a sign of GI colonization. Gummelsrud et al. observed higher intestinal Candida colonization rate in children with CF (7). Increased intestinal colonization is generally accepted as a major risk factor that predisposes high-risk patients to systemic candidiasis. Since the mortality risk is found to be similar in patients with multiple site fungal colonization, screening and relevant management is a matter of concern (30).
5.1. Conclusions
Candida albicans was the most frequent Candida species isolated from different specimens across all age groups and all wards, while the proportion made up by non-albicans Candida species was small. In our study, the low frequency of non-albicans Candida species such as C. glabrata and C. krusei may be resulted from the lack of national guidelines for antifungal prophylactic therapy, in Iran. We found that C. tropicalis and C. parapsilosis have emerged as important yeasts colonizing pediatric patients. Neonates and infants 1 - 12 months of age hospitalized in ICU, were more colonized by Candida species than other groups. Nonetheless, children admitted to general and surgical wards should be strictly monitored by a simple sampling from the respiratory, urinary, and intestinal tracts in order to enable detection of fungal colonization and prediction of subsequent infections.