







1. Background
2. Objectives
3. Methods
3.1. Bacterial Isolation and Identification
3.2. Inclusion/Exclusion Criteria
3.3. Antibiotic Susceptibility Testing
3.4. Carbonyl Cyanide m-Chlorophenyl Hydrazone
3.5. RNA Extraction and Real-time PCR
| Materials | Density | Volume Used (µL) |
|---|---|---|
| PCR master mix | 10 | |
| PCR buffer | 1x | |
| MgCl2 | 2 mM | |
| DNTPs | 0.4 mM | |
| Taq DNA polymerase | 0.2 u/μL | |
| Primers (F and R) | 0.8 μM | 0.5 |
| Template DNA | 0.5 μg/μL | 2 |
| Distilled water | - | 11 |
| Total volume | - | 25 |
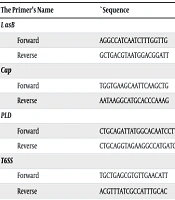
3.6. Identification of Pathogenic Genes
| The Primer’s Name | `Sequence | PCR Product Size (bp) | Reference |
|---|---|---|---|
| LasB | 137 | (14) | |
| Forward | AGGCCATCAATCTTTGGTTG | ||
| Reverse | GCTGACGTAATGGACGGATT | ||
| Cap | 211 | (15) | |
| Forward | TGGTGAAGCAATTCAAGCTG | ||
| Reverse | AATAAGGCATGCACCCAAAG | ||
| PLD | 1743 | (16) | |
| Forward | CTGCAGATTATGGCACAATCCTTTCATTCCA | ||
| Reverse | CTGCAGGTAGAAGGCCATGATGTAAAAAGTT | ||
| T6SS | 142 | (17) | |
| Forward | TGCTGAGCGTGTTGAACATT | ||
| Reverse | ACGTTTATCGCCATTTGCAC |
Abbreviations: Cap, capsule; PLD, phospholipase; T6SS, type VI secretion system.
| Primer Name | Sequence Primer | Size Primer (bp) | Product Size (bp) |
|---|---|---|---|
| 16S | 150 | ||
| Forward | CAGCTCGTGTCGTGAGATGT | 20 | |
| Reverse | CGTAAGGGCCATGATGACTT | 20 | |
| AdeB | 84 | ||
| Forward | AACGGACGACCATCTTTGAGTATT | 24 | |
| Reverse | CAGTTGTTCCATTTCACGCATT | 22 |
3.7. Ethical Statement
3.8. Sampling Method and Sample Size
3.9. Statistical Analysis
4. Results
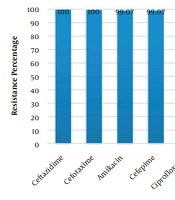
| Antibiotics | Sensitive | Intermediate | Resistant |
|---|---|---|---|
| AK | 2 (4.0) | 0 (0.0) | 48 (96.0) |
| GEN | 2 (4.0) | 2 (4.0) | 46 (92.0) |
| TN | 7 (14.0) | 2 (4.0) | 41 (82.0) |
| SAM | 2 (4.0) | 4 (8.0) | 44(88.0) |
| CPM | 0 (0.0) | 0 (0.0) | 50 (100) |
| Cefotaxime | 0 (0.0) | 0 (0.0) | 50 (100) |
| CAZ | 0 (0.0) | 0 (0.0) | 50 (100) |
| CIP | 1 (2.0) | 1 (2.0) | 48 (96.0) |
| Colistin | 40 (80.0) | 0 (0.0) | 10 (20.0) |
| IPM | 0 (0.0) | 0 (0.0) | 50 (100) |
| MEM | 0 (0.0) | 0 (0.0) | 50 (100) |
| PTZ | 0 (0.0) | 0 (0.0) | 50 (100) |
| MN | 14 (28.0) | 4 (8.0) | 32 (64.0) |
| Trimethoprim/sulfamethoxazole | 2 (4.0) | 1 (2.0) | 47 (94.0) |
Abbreviations: AK, amikacin; GEN, gentamicin; TN, tobramycin; SAM, ampicillin/sulbactam; CPM, cefepime; CAZ, ceftazidime; CIP, ciprofloxacin; IPM, imipenem; MEM, meropenem; PTZ, piperacillin/tazobactam; MN, minocycline.
a Values are expressed as No. (%).
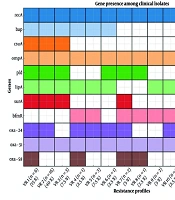
| Variables | OmpA | T6SS | Cap | LpsB | PLD | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Positive | Negative | P-Value | Positive | Negative | P-Value | Positive | Negative | P-Value | Positive | Negative | P-Value | Positive | Negative | P-Value | |
| AK | 1.00 | 1.00 | 0.49 | 0.07 | 1.00 | ||||||||||
| Sensitive | 1 | 1 | 2 | 0 | 2 | 0 | 1 | 1 | 2 | 0 | |||||
| Resistant/intermediate | 24 | 24 | 44 | 4 | 26 | 22 | 47 | 1 | 44 | 4 | |||||
| GEN | 0.49 | 1.00 | 1.00 | 0.07 | 1.00 | ||||||||||
| Sensitive | 0 | 2 | 2 | 0 | 1 | 1 | 1 | 1 | 2 | 0 | |||||
| Resistant/intermediate | 25 | 23 | 44 | 4 | 27 | 21 | 47 | 1 | 44 | 4 | |||||
| TN | 1.00 | 1.00 | 0.11 | 1.00 | 1.00 | ||||||||||
| Sensitive | 4 | 3 | 6 | 1 | 6 | 1 | 7 | 0 | 6 | 1 | |||||
| Resistant/intermediate | 21 | 22 | 40 | 3 | 22 | 21 | 41 | 2 | 40 | 3 | |||||
| SAM | 1.00 | 0.005 | 1.00 | 1.00 | 1.00 | ||||||||||
| Sensitive | 1 | 1 | 0 | 2 | 1 | 1 | 2 | 0 | 2 | 2 | |||||
| Resistant/intermediate | 24 | 24 | 46 | 2 | 27 | 21 | 46 | 2 | 44 | 4 | |||||
| CPM | N/A | N/A | N/A | N/A | N/A | ||||||||||
| Sensitive | 25 | 25 | 46 | 46 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Resistant/intermediate | 25 | 25 | 4 | 4 | 28 | 22 | 48 | 2 | 48 | 4 | |||||
| Cefotaxime | N/A | N/A | N/A | N/A | N/A | ||||||||||
| Sensitive | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Resistant/intermediate | 25 | 25 | 46 | 4 | 28 | 22 | 48 | 2 | 46 | 4 | |||||
| CAZ | N/A | N/A | N/A | N/A | N/A | ||||||||||
| Sensitive | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Resistant/intermediate | 25 | 25 | 46 | 4 | 28 | 22 | 48 | 2 | 46 | 4 | |||||
| CIP | 1.00 | 1.00 | 1.00 | 0.04 | 1.00 | ||||||||||
| Sensitive | 0 | 1 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 0 | |||||
| Resistant/intermediate | 25 | 24 | 45 | 4 | 27 | 22 | 48 | 1 | 45 | 4 | |||||
| Colistin | 0.07 | 0.17 | 0.48 | 1.00 | 0.17 | ||||||||||
| Sensitive | 23 | 17 | 38 | 2 | 21 | 19 | 38 | 2 | 38 | 2 | |||||
| Resistant/intermediate | 2 | 8 | 8 | 2 | 7 | 3 | 10 | 0 | 8 | 2 | |||||
| IPM | N/A | N/A | N/A | N/A | N/A | ||||||||||
| Sensitive | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Resistant/intermediate | 25 | 25 | 46 | 4 | 28 | 22 | 48 | 2 | 46 | 4 | |||||
| MEM | N/A | N/A | N/A | N/A | N/A | ||||||||||
| Sensitive | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Resistant/intermediate | 25 | 25 | 46 | 4 | 28 | 22 | 48 | 2 | 46 | 4 | |||||
| PTZ | N/A | N/A | N/A | N/A | N/A | ||||||||||
| Sensitive | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | |||||
| Resistant/intermediate | 25 | 25 | 46 | 4 | 28 | 22 | 48 | 2 | 46 | 4 | |||||
| MN | 0.11 | 1.00 | 0.53 | 1.00 | 1.00 | ||||||||||
| Sensitive | 10 | 4 | 13 | 1 | 9 | 5 | 13 | 1 | 13 | 1 | |||||
| Resistant/intermediate | 15 | 21 | 33 | 3 | 19 | 17 | 35 | 1 | 33 | 3 | |||||
| Trimethoprim/sulfamethoxazole | 0.49 | 0.15 | 1.00 | 1.00 | 0.15 | ||||||||||
| Sensitive | 0 | 2 | 1 | 1 | 1 | 1 | 2 | 0 | 1 | 1 | |||||
| Resistant/intermediate | 25 | 23 | 45 | 3 | 27 | 21 | 46 | 2 | 45 | 3 | |||||
Abbreviations: OmpA, outer membrane protein A; T6SS, type VI secretion system; Cap, capsule; LpsB, lipopolysaccharide biotinylated; PLD, phospholipase; AK, amikacin; GEN, gentamicin; TN, tobramycin; SAM, ampicillin/sulbactam; CPM, cefepime; CAZ, ceftazidime; CIP, ciprofloxacin; IPM, imipenem; MEM, meropenem; PTZ, piperacillin/tazobactam; MN, minocycline.
a N/A: No statistics were computed because those variables were constant.