

INTRODUCTION
METHODS AND SUBJECTS
Participants
Procedure
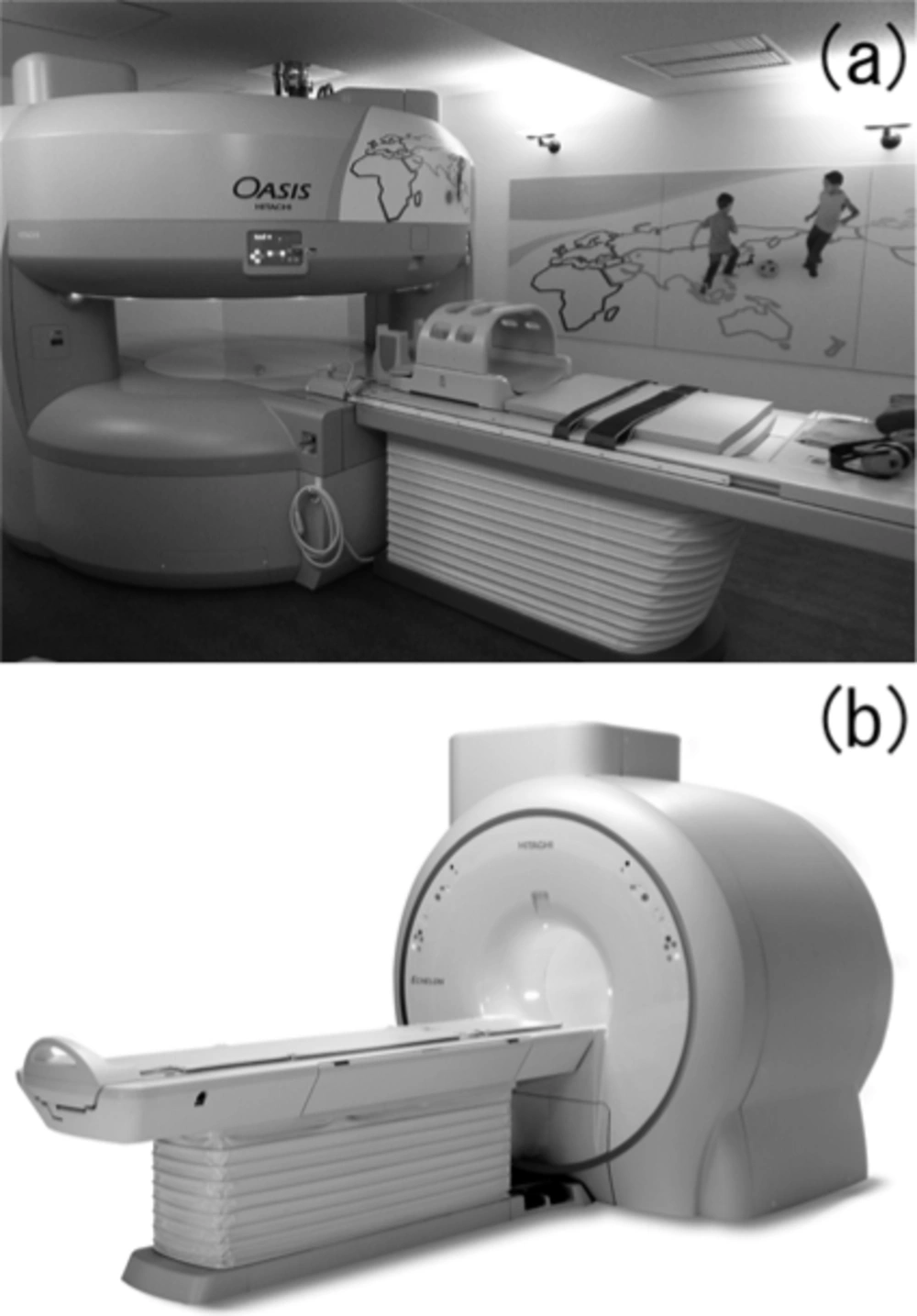
The configuration of two types of magnetic resonance systems: (a) the superconducting, horizontally opened, 1.2 T magnetic resonance system and (b) the conventional tunnel-type, bored 1.5 T magnetic resonance system.
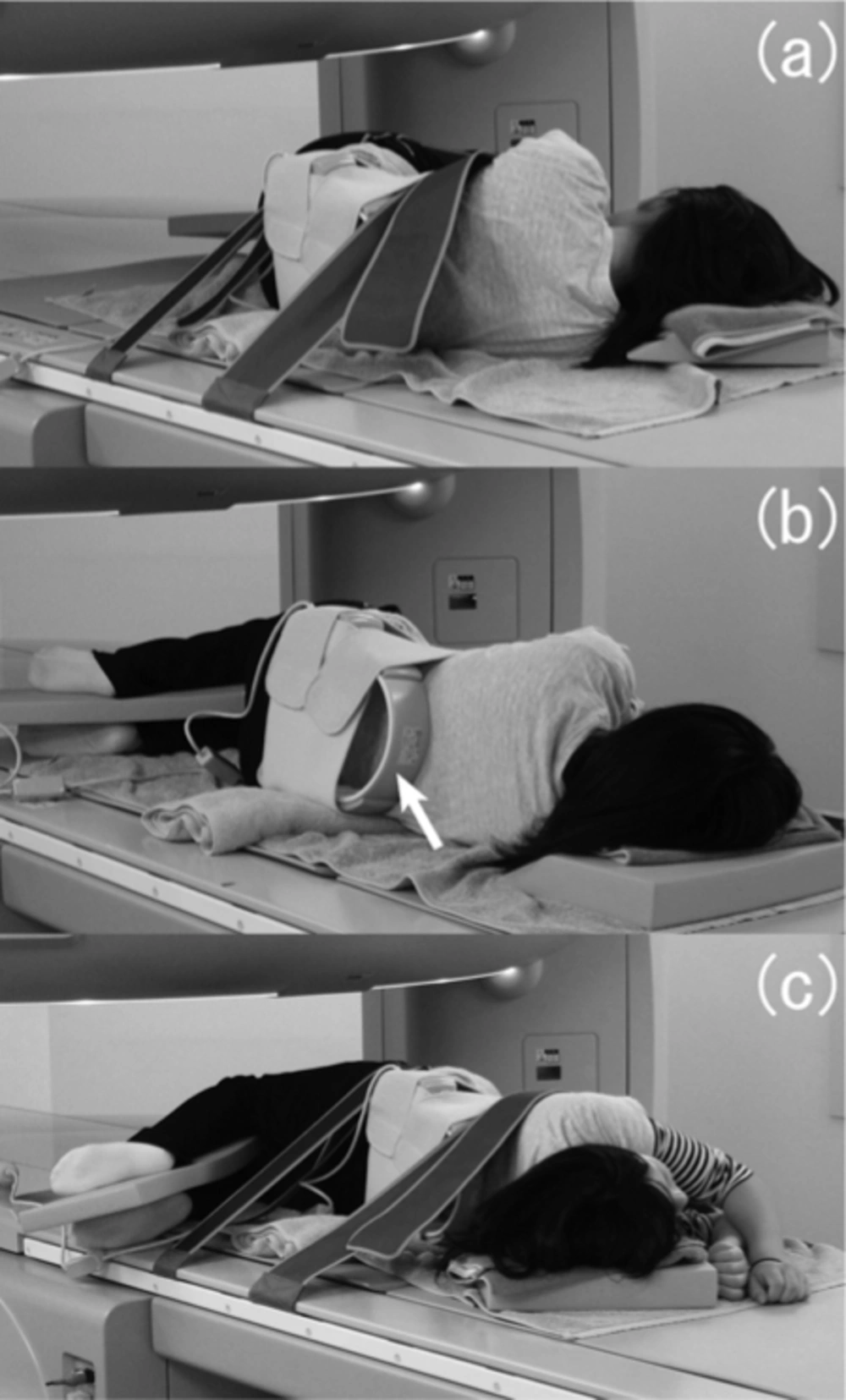
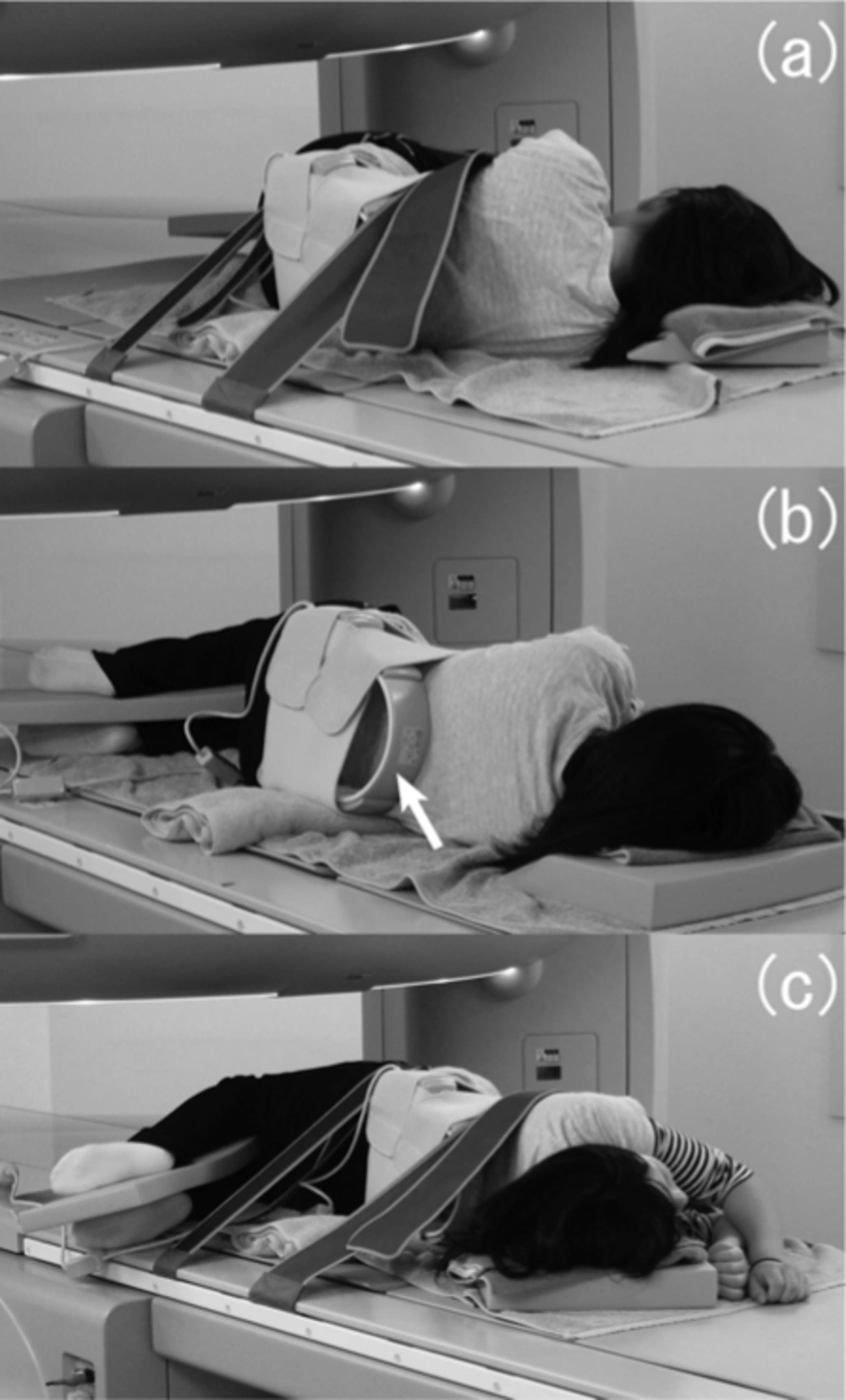
The postures in kinematic magnetic resonance imaging of the lumbar spine: (a) maximally anteflexed, (b) neutral, and (c) maximally retroflexed positions. A solenoid receiving coil was put on the subject's back (arrow).
The posture in kinematic magnetic resonance imaging of the knee. (a) The fixation of the knee by a supporting tool (CHAMCO, Inc., Cocoa, Florida, USA) and the arrangement of the solenoid receiving coil (arrow) are shown. The knee flexion can be adjusted from 0° to 120°. (b) The subject's position during the image acquisition is shown.
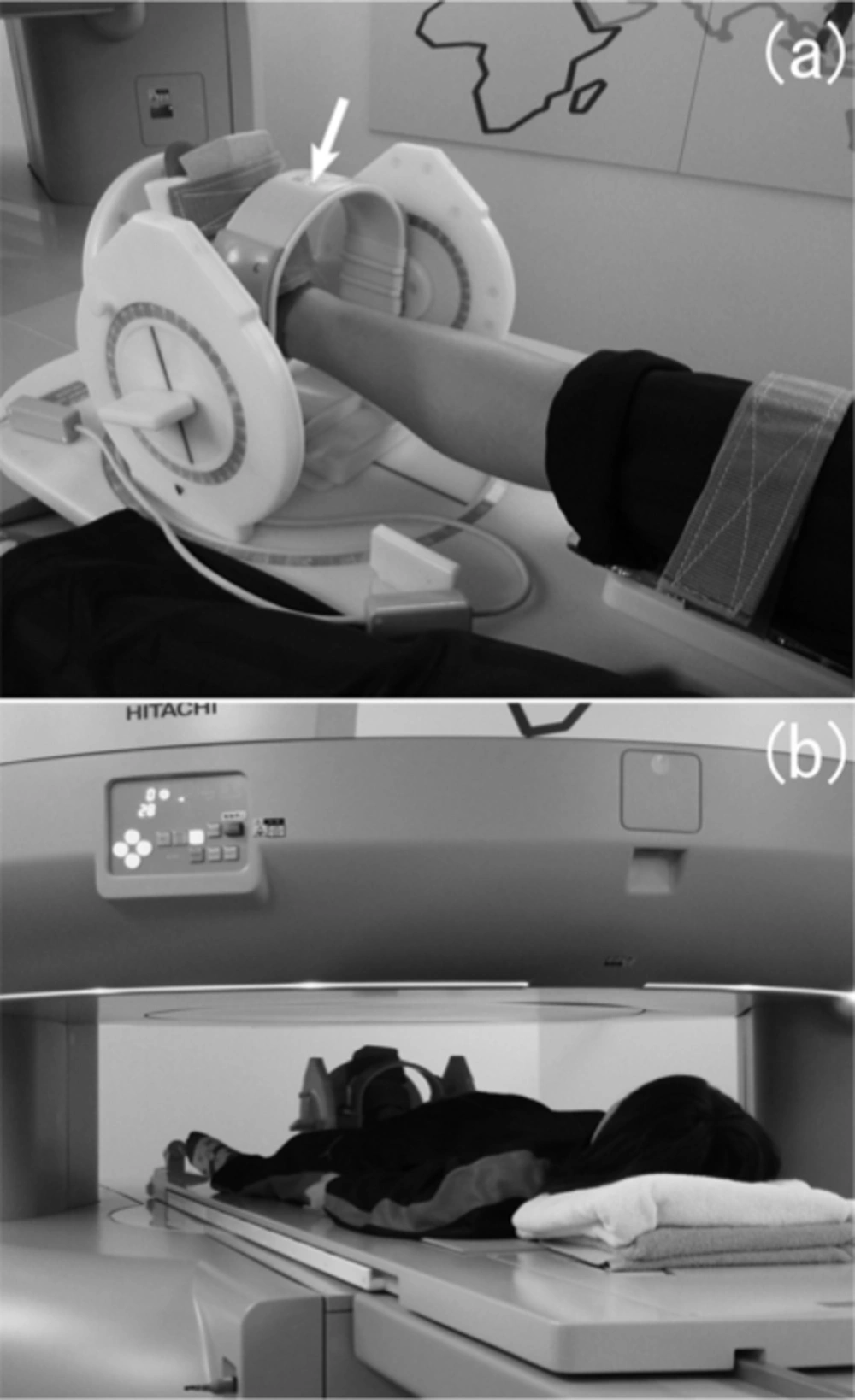
The posture in kinematic magnetic resonance imaging of the ankle. (a) The fixation of the ankle by a supporting tool (CHAMCO, Inc., Cocoa, Florida, USA) and the arrangement of the solenoid receiving coil (arrow) are shown. (b) The subject's position during the image acquisition is shown.
RESULTS
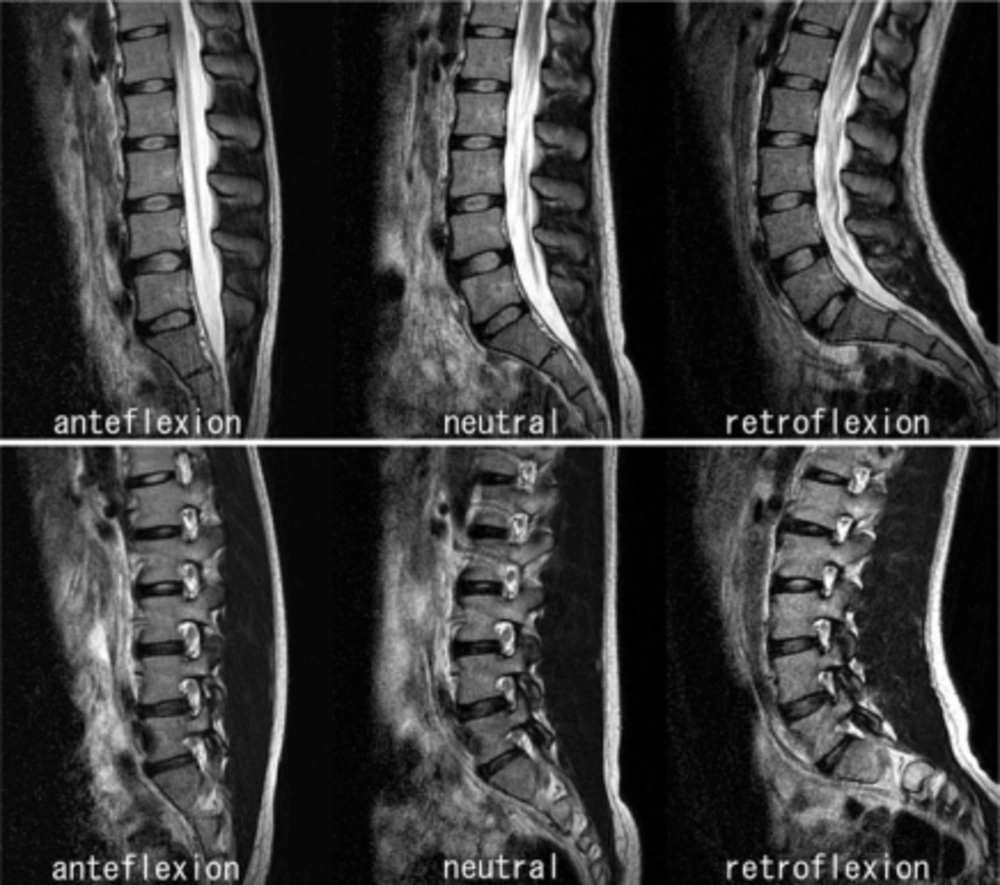
Example of kinematic magnetic resonance images of the lumbar spine. Upper row: slices at the middle plane of the vertebral body. Lower row: slices at the level of the intervertebral foramen. Each of them is arranged from left to right in order of maximal anteflexion, neutral, and maximal retroflexion positions.
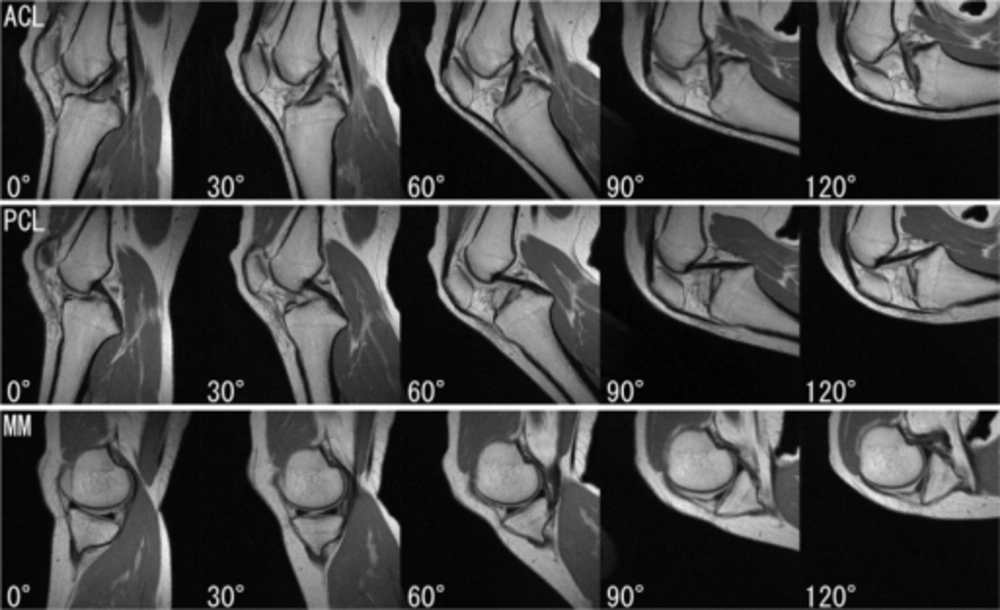
Example of kinematic magnetic resonance images of the knee. Upper row: slices at the level of the anterior cruciate ligament (ACL). Middle row: slices at the level of the posterior cruciate ligament (PCL). Lower row: slices at the level of the medial meniscus (MM). The angle indicated at the lower left of each image is the flexion angle of the knee.
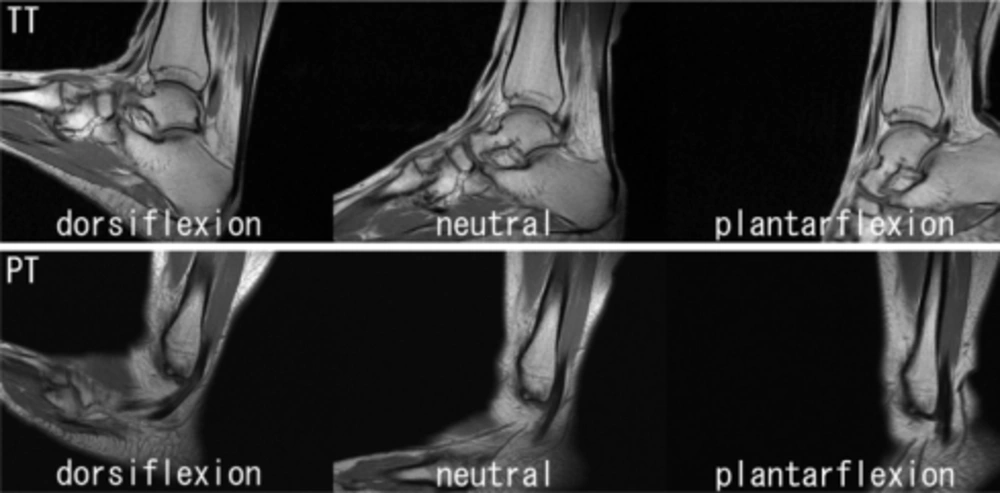
Example of kinematic magnetic resonance images of the ankle. Upper row: slices at the central trochlea of the talus (TT). Lower row: slices at the level of the peroneal tendon (PT). Each of them is arranged in order from left to right of maximal dorsiflexion, neutral, and maximal plantarflexion positions.

