This study aimed to evaluate the antimicrobial resistance and infection risks in Tertiary hospitals in Benin. The tertiaries hospitals of Sakété-Ifangni and Menontin were chosen as the study cases. The evaluation of the infection risk at Sakété-Ifangni hospital showed the presence of SCN (45%) as the predominant species, followed by
Staphylococcus aureus (27.50%) and
Pseudomonas aeruginosa (15%). Many other studies highlighted the role of these pathogens in the contamination of surfaces and nosocomial infections (
6,
7,
9). Even if our study agrees with the study by Afle et al. (
17), as regards the presence of these germs, they differ in the prevalence of germs found. Indeed, this study revealed the predominance of
Staphylococcus aureus,
Klebsiella spp., and
Acinetobacter baumannii.
Klebsiella pneumoniae,
Escherichia coli, and
Enterobacter cloacae were the predominant germs found in the environment of the National University Hospital Center HKM of Cotonou (
15). These discrepancies show the diversity of pathogens involved in contamination according to the hospital center. It would, therefore, be important to establish a map of germs according to health centers in order to better control the spread of multidrug-resistant bacteria responsible for infections associated with healthcare settings. The study of antibiotic resistance showed numerous resistant strains in accordance with the literature (
21,
22). The strong presence of SCN is an indicator of poor hand hygiene. The study by Degbey et al. in 2016 (
14) already highlighted the poor quality of hand hygiene among health professionals in Benin, but it is well known that hand hygiene alone can reduce 80% of the frequency of infections. It is important that these health professionals adopt good practices in the healthcare setting (
23).
Out of 60 festering wounds swabbed at Menontin Hospital, 59 showed the presence of at least one bacterium. Moreover, 75% of wound pus samples contained two bacterial strains. The production of pus by wounds is the most visible sign of colonization of the wounds by bacteria. Therefore, wounds can be contaminated by microorganisms that colonize the surfaces and air. In this hospital, the material used during dressing (pliers, compress, scissors, beans, and trays) was contaminated, which highlights the problem of sterilization and preservation of the sterilized material. These results corroborate those obtained by Degbey et al. in 2013 (
13) in a study on the quality of technical medical equipment used in the operating theaters of the Center National Hospitalier Universitaire HKM de Cotonou. A study by Slekovec et al. (
24) showed that wound care is also a source of contamination of surfaces and equipment that can spread to subsequent patients. It is, therefore, a source of the spread of infections within hospitals. These hospitals need to incorporate good bio-cleaning and sterilization techniques for technical medical equipment into their programs in order to control the risk of infection in hospitals. Among the bacteria involved in the suppuration of the wounds, we mostly isolated
Staphylococcus aureus (31%), followed by
Escherichia coli (15%) and coagulase-negative staphylococci (12%). They are the bacteria encountered in nosocomial infections, in general, and in wound infections, in particular (
24,
25). The multi-resistant nature of the isolated strains is also in agreement with the hospital origin of the strains because the hospital strains are well known for their multi-resistance (
21). The comparison of the resistance profiles showed that there were the same profiles of circulating strains in the environment and wounds. The resistance proportions obtained for bacteria isolated from wounds and the environment in the present study are close to those of bacteria isolated from wounds and the environment at the University Hospital of Mother and Child-Lagoon (
16). This study, therefore, confirms the role of the environment, especially the collection rooms, in the colonization of wounds in patients. It also shows that the issue of antimicrobial resistance is the same reality in health centers regardless of levels.
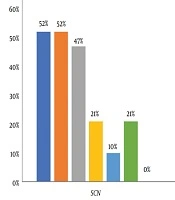
The study of the adequacy of the treatment showed that for 38% of the infected wounds, no antibiotic treatment was administered and 10% of treatment was contrary to the result of the antibiogram. Indeed, the action of antiseptics is limited to the bacteria present during the operation although the good quality of antibiotics is needed. The inappropriate use of antibiotics without screening is likely to increase the incidence of multidrug-resistant bacteria. These results reveal a problem in the prescription of antibiotics in hospitals. Indeed, the prescription of antibiotics requires a good diagnostic approach including the establishment of an etiological diagnosis either by the isolation and identification of the infectious agent or by serological tests to establish contact with the pathogen. Ouedraogo et al. (
26). Therefore, before any antibiotic prescription to an injured patient, it is important to carry out bacteriological examinations of wound swabs to provide adequate management of wound superinfections by multidrug-resistant bacteria.