1. Background
Celiac disease (CD) is an enteropathy with permanent sensitivity to gluten in genetically susceptible subjects. Clinical manifestations of CD are highly variable and include gastrointestinal or extra-intestinal symptoms. Extra-intestinal manifestations in children with CD include short stature, dermatitis herpetiformis, arthritis, osteoporosis, and iron deficiency anemia (1).
In addition, there are also a number of manifestations of CD that affect the oral cavity. These include dental enamel defects affecting predominantly the secondary teeth, recurrent aphthous stomatitis (RAS), delayed tooth eruption, and xerostomia (2). Dental enamel defects (DED) are reported to be more common in children and adults with CD compared to the general population, and may occur in the absence of gastrointestinal symptoms (3). In a recent systematic review of extra-intestinal manifestations of CD, including 2840 patients, the prevalence of dental enamel defects in people with CD was 50% (4). In a study by Wierink et al. on 53 Dutch children with proven CD, 55% had enamel defects compared to 18% in control subjects (5). In another study involving 27 children with CD and 27 healthy subjects, Priovolou et al. found enamel defects using the Aine criteria to be more common in CD than controls. These authors concluded that while CD increases the risk of developing enamel defects in permanent teeth, it did not increase the risk for dental caries (6). Although impaired dental mineralization may occur in other systemic diseases, enamel defects are felt to be specific to CD when they are symmetrically distributed and detectable in all four quadrants of the dentition (2, 5).
This study aimed to determine the prevalence of dental enamel defects, dental caries, and other oral manifestations in a group of Iranian children with CD and compare them to a group of children without CD. Early detection of dental changes may serve as a valuable means for identifying children who need to be tested for CD.
2. Methods
2.1. Study Population
The study was offered to 200 index cases with celiac disease as an oral explanation for the family during the visit to assess their willingness for participation. From 200 index cases, 65 children with celiac disease accepted to participated in the research. The study was carried out in the pediatric gastroenterology and dentistry units at a teaching hospital. Diagnosis of 65 children with celiac disease was confirmed by compatible serologic tests, characteristic small bowel intestinal histology, and response to a gluten free diet according to the ESPGHAN criteria (7). In addition, 60 healthy subjects who requested routine dental checkup were included as a control group. After obtaining consent, all children in the control group were checked for TTG-IgA and total serum IgA levels, which had normal levels. Children with any other systemic diseases associated with enamel changes, using medications such as tetracycline, premature delivery, trauma to teeth, and CNS problems were excluded from the study. Teeth that were fractured, had large carious lesions, or had restoration involving more than two-thirds of the dental surface were excluded from the evaluation.
Informed consent was obtained from the children and their parents. A questionnaire was completed by researchers of the study through face-to-face interviews with parents and subjects to obtain demographic characteristics, educational level of parents, family income, past medical history, age of initiation of gluten free diet, history of trauma to teeth, tooth brushing habits, daily sugar usage, recurrent aphthous ulcers, xerostomia, and tongue burning. Results of TTG IgA, and total serum IgA levels and, in the CD children, the biopsy findings were recorded. Anthropometric measurements based on the WHO Global Database on child growth and malnutrition, which utilizes a Z-score cut-off point of < -2 SD to classify low weight-for-age and height-for-age, was used to define underweight and stunting (8).
2.2. Oral Assessment
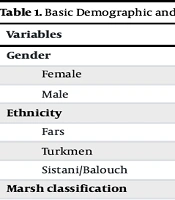
Examinations were carried out in a dentistry room with dental equipment and using artificial light together with a forehead lamp. All examinations were carried out by a single dentist who was blinded as to which group the child belonged to and was trained to assess enamel defects and dental caries in children. After thorough cleaning and drying of the teeth, the oral cavity was carefully examined for dental enamel defects, caries, and delay in eruption as well as for any soft tissue lesions (RAS, atrophic glossitis, geographic tongue). The location and coronal distribution of enamel defects and number of affected teeth was recorded. Enamel defects in deciduous and permanent teeth were assigned a grade from 0 to IV, according to the Aine criteria (3) (Table 1). DMFT/dmft scores were recorded by calculating the number of decayed (D), missing (M), and filled (F) teeth in the dentition (8). Enamel defects were considered to be specific for CD if they were symmetrically distributed and detectable in all four quadrants of the dentition; whereas non-specific enamel defects occur symmetrically and chronologically but involve the superior and inferior hemi-arches on the same side (5). Both specific and non-specific enamel defects were recorded. The study was approved by the Ethics Committee of Children and Adolescents Health Research Center, Resistant Tuberculosis Institute, Zahedan University of Medical Sciences.
Table 1.Classification of Dental Enamel Defect Based on the Aine Criteria
| Grade | Defect |
|---|---|
| 0 | No defects |
| 1 | Defect in enamel color |
| 2 | Slight structural defects. Rough enamel surface, horizontal grooves, or shallow pits |
| 3 | Evident structural defects. Rough enamel surface filled with deep horizontal grooves of variable width or having large vertical pits. Large opacities of different colors or strong discoloration may be combined. |
| 4 | Severe structural defects. The shape of the tooth is changed, tips of cusps are sharp-pointed and/or incisal edges are thinned and rough. Thinning of the enamel is readily detected and the margins of the lesions are well defined. The lesion may be strongly discolored. |
Statistical Analysis: The data were analyzed using SPSS.18 (Chicago, SPSS Inc.) and significance level was defined as P < 0.05. Chi-Square test and Mann-Whitney test were used for comparison of data.
3. Results
Table 2 compares the two groups for some of the recorded variables. There were 65 children with CD (ages three to16 years, 42 female) and 60 subjects in the control group (ages three to 16 years, 29 female). There were no significant differences between the two groups with regards to educational level or income of the parents. More children in the CD group were undernourished compared to the control group (66% vs. 34%, P = 0.03). In additino, dmft index was significantly higher in children with celiac disease compared with the control group (P = 0.03). Children with CD were more likely to have xerostomia and were less likely to have high daily sugar intake than those without CD (Table 2).
Table 2.Comparison of Variables Between Celiac and Control Groupsa
| Variables | Celiac | Control | P Valueb |
|---|---|---|---|
| Underweight | 27 (66) | 14 (34) | 0.03c |
| Stunting | 19 (63.3) | 11 (36.7) | 0.1c |
| DMFT, mean ± SD | 0.7 ± 1.5 | 0.6 ± 1.2 | 0.8d |
| dmft, mean ± SD | 5.1 ± 4.6 | 2.4 ± 2.6 | 0.003d |
| No tooth brushing | 29 (45) | 36 (55) | 0.06c |
| Sugar usage > 3 times/day | 16 (25) | 28 (47) | 0.001c |
| Recurrent aphthous ulcers | 11 (17) | 8 (13) | 0.3c |
| Xerostosis | 10 (15.4) | 3 (5) | 0.05c |
| Tongue burning | 8 (12) | 2 (3) | 0.06c |
a Values are expressed as No. (%) unless otherwise indicated.
b P value < 0.05 is significant.
c Chi-Square.
d Mann-Whitney test.
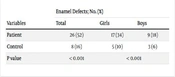
There were significantly more enamel defects in children with CD compared to the control group (Table 3, P = 0.01). Grade I was the most common enamel defect in both groups whereas only children with CD had grade 3 and 4 defects. Symmetric and non-symmetric enamel defects were observed in 45% and 14% of CD subjects and in 12% and 12% of the control group, respectively. The prevalence of symmetrical defects was significantly greater in children with CD (P = 0.01, Table 3). Enamel defects were more prominent in the anterior teeth with the incisors and canines most commonly affected. In addition, there was a coronal distribution to the defects with the incisor surface and middle portions of the teeth most prominently involved. There was no effect of gender or age on the prevalence of enamel defects.
Table 3.Dental Enamel Defect (DED) Based on Aine Classificationa
| Classification and Grade of DED | Control | CD | P Value |
|---|---|---|---|
| Symmetric ED | 7 (12) | 29 (45) | 0.001 |
| Non-symmetric ED | 7 (12) | 9 (14) | 0.001 |
| Enamel defect | 0.001 | ||
| Grade 1 | 9 (15.0) | 27 (41.5) | |
| Grade 2 | 4 (6.7) | 8 (12.3) | |
| Grade 3 | 0 | 3 (4.6) | |
| Grade 4 | 0 | 1 (1.5) |
a Values are expressed as No. (%).
4. Discussion
Dental enamel defects have been reported in children with CD, although the prevalence varies between geographical regions (Table 4). In patients with undiagnosed CD, dental and oral manifestations such as enamel defects, delayed eruption of teeth, and recurrent aphthous ulcers can sometimes be the only initial presenting manifestations (9, 10). In some European countries, dentists are known to refer children for testing for CD on the basis of finding dental enamel defects during routine dental visits. Currently, no such practice occurs in Iran, which is probably due to the fact that dental enamel defects are not recognized as a manifestation of CD in this country. This study now demonstrates that the typical enamel defects that are symmetrically distributed in CD are a relatively common finding in children with CD in Iran and were present in almost 50% of those with a confirmed diagnosis of CD compared to only 12% of children without the condition. In contrast, dental caries involving the secondary dentition was no more common in children with CD compared to the control group.
Table 4.Prevalence of Dental Enamel Defects in Different Studies
| Authors | Year | Reference | Number of Subjects | CD / Control | Grade (%) | ||
|---|---|---|---|---|---|---|---|
| Celiac | Control | DED (%) | Symmetric / Non - Symmetric (%) | ||||
| Aine et al. | 1990 | (3) | 40 | 112 | 69 / 19 | 83 / 4 | II (53) |
| Aguirre et al. | 1997 | (11) | 137 | 52 | 52 / 42 | 72 / 41 | - |
| Costacurta et al. | 2010 | (12) | 300 | 300 | 33 / 11 | 60 / 15 | I (80) |
| Avsar and Kalayci | 2008 | (13) | 64 | 64 | 42 / 9 | 42 / 9 | I (20) |
| Priovolou et al. | 2004 | (6) | 27 | 27 | 83 / 50 | 44 / 11 | I (70) |
| Procaccini et al. | 2007 | (14) | 50 | 50 | 26 / 16 | - | I (76) |
| Cantekin et al. | 2015 | (15) | 25 | 25 | 48 / 16 | Most | - |
| Wierink et al. | 2007 | (5) | 53 | 28 | 55 /18 | 38 / 4 | - |
| Ortega Paez et al. | 2008 | (16) | 30 | 30 | 83 / 53 | 73 / 23 | I (44) |
| de Carvalho et al. | 2015 | (17) | 52 | 52 | 61 / 21 | 58 / 13 | I (44) |
| Present study | 65 | 60 | 60 / 22 | 45 / 12 | I (15) | ||
The mechanism leading to enamel defects in CD subjects is not fully understood with nutritional, genetic, and immunological factors all being implicated. Hypocalcemia, secondary to intestinal malabsorption in CD may play a role (18), and a lower serum calcium level in those with DED was considered an important predictor of CD in one study (19). Conversely no such relationship between calcium levels and DED was found in another study (13). Moreover, hypocalcemia is questionable after observing no significant differences in serum calcium concentrations in children with deciduous teeth (20). The involvement of deciduous teeth in this study supports the hypothesis that immunologic and genetic factors play a more prominent role in the onset of DED than nutritional factors as mineralization of deciduous teeth is completed in utero (20). In support of an autoimmune pathogenesis for DED in CD is the fact that enamel defects are also present in other autoimmune diseases, are associated with certain HLA haplotypes (20, 21), and may found in healthy first-degree relatives of subjects with celiac disease (22).
The prevalence of enamel defects in children with CD has been reported in 38% to 96% of cases and many studies have shown DED to be more prevalent in CD patients compared to healthy individuals (5, 6, 13, 23). As a result the presence of enamel defects and/or aphthous stomatitis in a child is now considered by some to be an indication to test for CD (24). However, others have not found DED to be more common in CD (12, 25) and dental enamel defects are not specific to CD as they can occur secondary to other conditions such as dental fluorosis or tetracycline therapy (26). Our study supports the association between CD and DED and, although much less than the 96% was reported by Aine (27), we identified almost 50% of children with CD having the characteristic symmetrical distribution of DED. The majority only had Grade I defects, however, in a small number, the defects were severe (Grades 3 and 4). Our findings are similar to those reported elsewhere (6, 16), and in contrast to those reported by Aine who found most Finnish children had Grade 2 defects with 30% having Grade 4 defects. The reasons for these differences is not clear, however, it could be related to the fact that children in Aine’s study were generally older at the time of diagnosis of their CD.
A number of studies have evaluated DMFT/dmft scores as a measure of caries in children with CD compared to those without this condition. Some report caries to be more frequent in CD (12, 15) while others have shown the opposite relationship (6, 28). In our study a higher caries index in only deciduous teeth was observed. A possible explanation for this finding includes the higher sugar consumption recorded in the control subjects. It did not appear to be related to differences in dental hygiene between the two groups. Given the high number of children with dental caries and high frequency of celiac disease in children and their families in our region (29-31), further attention to public dental care programs and screening of celiac disease is recommended.
Regarding the location of the CD-related DEDs, incisors and canines were the areas most involved in permanent and deciduous teeth, respectively. This distribution could be explained by the chronology of formation of deciduous and permanent teeth. Studies in permanent teeth demonstrate that molars, followed by incisors, then canines, are the order in which the mineralization process progresses (2). The coronal distribution of enamel defects in our study, with the incisor and middle parts of the teeth being most affected, is similar to the findings by Ortega Paez et al., and could be attributed to time relationship between etiologic factors and odontogenesis (16).
With regards to other non-dental oral findings, only the presence of xerostomia was found to be more common in children with CD compared to the control group. A number of studies have shown RAS to be more frequent in children with CD compared to those who do not have the condition (14, 15, 17, 32). The percentage of children with RAS in our study was higher among the CD group, however, this did not reach the level of statistical significance. The cause of aphthous ulcers in CD is unknown, however, it may be related to malabsorption of nutrients such as iron, folic acid, and vitamin B12 (21).
In conclusion, this study demonstrates that symmetrical DED are a relatively common finding in children with CD as compared to those without CD. As such, the presence of such defects should serve to alert health care providers to the possibility that the child may have CD and should be considered for testing. A limitation of this study was the relatively small number of subjects in each group. On the other hand, strengths of this study are that only confirmed cases of CD were compared to those in whom CD had been excluded and that the dentist was blinded as to which group the child belonged to. Never-the-less, the difference in prevalence of symmetrical DED was large enough to suggest this is a relevant finding. As in many other parts of the world, CD is under diagnosed in Iran in part due to a failure by health care providers to recognize the highly varied manifestations of this condition. An increased awareness of the oral manifestations of CD will hopefully lead to a timelier diagnosis of CD in some children.