In the present study, we aimed to compare the prevalence of MetS in women with a history of CS or NVD. The study of metabolic syndrome and the factors influencing it after childbirth is of great importance given the rising prevalence of obesity and metabolic syndrome in women (
24). In this study, 30% of mothers who underwent CS and 18% of mothers with a history of NVD were identified with MetS. Studies have revealed that an increase in maternal BMI is also linked to a rise in emergency CS delivery rates (
17,
25-
27). Research has indicated that CS is associated with slight increases in blood pressure, BMI, and fat mass, but not with other metabolic risk factors (
28). Metabolic syndrome is connected to various reproductive factors, such as the onset of menarche, the number of births, and the age at first birth (
29). However, to our knowledge, this is the first study to investigate the relationship between mode of delivery and metabolic syndrome in women.
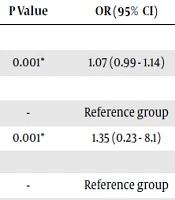
The OR of developing MetS in women with a history of CS was nearly double that of mothers who had NVD. Specifically, the OR for developing MetS in women with NVD was found to be 0.57, indicating a 33% lower likelihood of MetS in these women compared to those who underwent CS. This finding suggests that NVD may be a protective factor against MetS. Despite this result, we did not find any studies directly linking metabolic syndrome to mode of delivery. Abdominal obesity following cesarean delivery is one factor that may explain the higher rate of MetS among women who delivered via this method. Studies indicate that visceral and intra-abdominal fat, unlike subcutaneous fat, can promote inflammation. Additionally, abdominal fat has been linked with insulin resistance, leading to a higher concentration of toxic free fatty acids in the portal blood flow, which predisposes women to metabolic syndrome (
16,
17,
19). Abdominal obesity is also associated with an increased risk of hypertension, pre-diabetes, diabetes, and cardiovascular events, all of which are risk factors for metabolic syndrome (
20,
21).
Mothers who had NVD and did not have MetS were found to have a longer duration of breastfeeding. Our findings align with a cross-sectional study conducted in Poland, which indicated that women who breastfed had a lower rate of MetS (
30). Similarly, the Tehran Lipid and Glucose Study demonstrated that women may be more protected against MetS if they breastfeed for up to 12 months (
31). However, another study conducted three years postpartum found no dose-response relationship between the duration of lactation and MetS (
32). These varying results may be attributed to factors such as selection bias, differences in study timeframes, declines in breastfeeding rates, or unmeasured biomarkers in the studies.
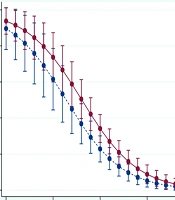
Univariate analysis in our study revealed that both breastfeeding and NVD were strongly associated with a reduced risk of MetS. Specifically, the duration of breastfeeding was significantly linked to a decreased likelihood of MetS, with each additional year of breastfeeding lowering the risk by nearly 30%. The prevalence of MetS was higher among women with a history of CS delivery compared to those with NVD. Importantly, we found that the difference in MetS prevalence between the two delivery methods diminished with an increase in breastfeeding duration. Notably, mothers who breastfed for more than 20 months in either group had zero prevalence of MetS.
Additionally, other studies have reported that breastfeeding has a protective effect against the development of MetS after delivery, with breastfeeding for 1 to 1.5 years significantly reducing the risk (
31). Experimental research has also indicated that not breastfeeding may be associated with weight gain (
33), obesity (
34), and MetS (
35) postpartum.
Altogether, women with a history of cesarean section are advised to follow healthcare guidance and undergo appropriate preventive measures to reduce the risk of abdominal obesity and MetS.
Our study has several limitations. First, its cross-sectional design limits the ability to infer causal relationships. Secondly, while we found an association between metabolic syndrome and mode of delivery, it is important to determine whether this relationship is causal or influenced by confounding factors. Third, the small sample size necessitates caution when interpreting the results.
5.1. Conclusion
This study found that women who had undergone cesarean section were more likely to develop metabolic syndrome compared to those who had natural vaginal delivery (NVD). Since we did not assess or compare certain confounding variables, such as BMI, waist circumference, and lipid levels between the NVD and CS groups at the time of delivery, we cannot rule out their influence on the results. Therefore, we cannot definitively conclude that mode of delivery is a direct predictor of MetS. Additionally, our findings suggest that increased breastfeeding duration and the choice of NVD are associated with a lower likelihood of MetS. As a result, obstetricians and midwives should consider the potential risk of MetS when deciding whether to perform elective CS. Moreover, planning to reduce the rate of unnecessary cesarean sections is recommended.







")