1. Background
Chronic kidney disease (CKD) is a worldwide public health problem. End-stage renal disease (ESRD) substantially increases the risks of death, cardiovascular diseases, and use of specialized health care (1). The number of patients enrolled in the ESRD Medicare-funded program increased from approximately 10,000 beneficiaries in 1973 to 86,354 in 1983, and 547,982 as of December 31, 2008 (2). Malnutrition is a relatively common problem in patients undergoing hemodialysis and is also associated with increased morbidity and mortality in the affected patients, as described in a recent Dialysis Outcomes Quality Initiative (DOQI) (1). Nutritional assessment can be done by anthropometric measurements, laboratory parameters, subjective global assessment, dialysis malnutrition score, near infra-red interactance, and other methods. Subjective global assessment is currently the most accepted one which classifies patients into three nutritional categories: Well nourished, moderately malnourished, and severely malnourished (3). There is no specific measure which can be used in all patient populations to accurately assess nutritional status. This is particularly true in renal failure which can alter the plasma levels of some parameters used to estimate nutrition. The criteria to diagnose protein-energy wasting include a serum albumin of less than 3.8 g/L, serum pre-albumin of less than 30 mg/dL, and serum cholesterol less than 100 mg/dL. A number of body mass measures, such as BMI, anthropometry, dietary protein, and energy intake may also be used to identify the presence of protein-energy wasting. Thus, patients with ESRD, like other patients, should undergo a variety of measurements to develop a profile to detect the possible development of malnutrition (4). Several studies demonstrated a negative correlation between the plasma albumin concentration and mortality in patients undergoing maintenance hemodialysis or peritoneal dialysis (5, 6). The increase in mortality with hypoalbuminemia appears to occur even at near normal albumin levels (3.5 g/dL); however, the risk is greater with more severe hypoalbuminemia, being the greatest in patients with a plasma albumin concentration below 3 g/dL (5). A serum albumin concentration less than 3.8 g/L suggests a diagnosis of protein-energy wasting (7).
2. Objectives
The current study mainly aimed to investigate the relationship between nutritional markers, anthropometric parameters such as BMI, and routine laboratory parameters with mortality in patients undergoing hemodialysis.
3. Materials and Methods
3.1. Patients and Study Design
The current study was approved by the Ethics Committee of the Ardabil University of Medical Sciences. It was an observational retrospective cross-sectional study carried out in the hemodialysis center of Bu-Ali Hospital, the largest hemodialysis center hospital in Ardabil City, Iran. The duration of the study was a period of 11 years from May 2001 to July 2011. A total of 260 patients undergoing hemodialysis with end-stage chronic kidney disease were enrolled in the study. Inclusion criteria for all patients were: hemodialysis treatment for at least the previous 6 months, 3 times a week, for at least 4 hours per session, with the dialysis dose being mediated by ionic conductivity Kt/V > 1.5 and at least 18 years old. Patients with acute pathologies and those who had to be hospitalized within the last three months were excluded. A questionnaire was used to collect the following data from each participant: age, gender, and body weight before hemodialysis, height, BMI, body weight after hemodialysis, and the existence of any underlying previous diseases. Biochemical measurements were routinely drawn once every three months. It included serum potassium, phosphorus, calcium bicarbonate, parathyroid hormone (PTH), albumin, total protein, triglyceride, cholesterol, blood urea nitrogen (BUN), and Creatinine. All participants signed an informed consent form and declared their willingness to allow the application of their anonymous data for research purposes. The patients were regularly followed-up for one year. Lastly, the year follow-up was completed by 90 patients.
3.2. Statistical Analysis
The collected data were analyzed using SPSS software (Version 19.SPSS Inc. United States). Student’s t test and chi-square test were used to compare continuous and categorical variables, respectively. The Pearson correlation analysis was used to evaluate the correlation between scores of the different scales and other relevant variables. P < 0.05 was considered as level of significant. The results were expressed as means ± standard deviations.
4. Results
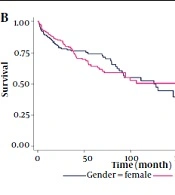
In the current analysis included 260 patients undergoing hemodialysis (140 male and 120 female). Lastly, the year follow-up was completed by 90 patients (52 male and 38 female); the causes of loss to follow-up were: death (n = 150), transplantation (n = 4), transfer to peritoneal dialysis (n = 2), change of dialysis center (n = 3), and other causes (n = 11). The mean age of alive patients was 56.8 ± 10.6 years and the mean age of dead patients was 54.8 ± 7.8 years. The patient and control groups were not significantly different regarding age and gender (P = 0.911) (Table 1). Age of dialysis onset in alive patients (54.94 ± 14.3 years) was less than that of the dead patients (61.75 ± 14.15 years). The mean age of female and male patients were 61.63 ± 13.16, and 57.73 ± 15.22 years, respectively, which was statistically significant (P = 0.032) (Table 2). The mean duration of dialysis in the patients was 33.03± 27.91 months. The mean duration of hemodialysis in the alive and dead patients were 42.85 ± 30.71 and 26.27 ± 23.74 months, respectively, which were statistically significant (P = 0.001). The patients were divided into four categories on the basis of their baseline BMI: < 19, 19 to 25, 25 to 30, and ≥ 30 kg/m2; 10% of the patients had a BMI less than 19 Kg/m2, 56.9% between 19-25 kg/m2, 26.2% between 25-30 kg/m2, and 6.9% ≥30 kg/m2. There was no significant difference between BMI and the life status (P = 0.654) (Table 3). The biochemical measurements in alive and dead patients are shown in table 3. ANOVA test results proved no significant difference regarding the means of serum triglyceride, cholesterol and BUN between alive and dead patients. However, there was a correlation between serum albumin and creatinine in alive and dead patients and the difference was statistically significant (P value: 0.001 and 0.034, respectively). The current study reviewed the relationship between gender and biochemical measurements. The obtained results showed that the mean levels of serum albumin, triglyceride and cholesterol were more in women than in men and the difference was statistically significant (Table 4), but the mean serum BUN and creatinine levels were more in men than in women, but the difference was not statistically significant. Finally, the study reviewed the studied variables (gender, dialysis duration, BMI, albumin, triglyceride, cholesterol, urea, and creatinine) using linear regression analysis. The results showed that only the serum levels of albumin and dialysis duration had the statistical significant differences between alive and dead patients (Table 5).
Table 1.
The Relationship Between Survival Status of the Patients and Gender a
| Gender | Number of Alive Patients | Number of Dead Patients | P Value |
|---|---|---|---|
| Male | 52 (57.8) | 97 (57.1) | 0.911 |
| Female | 38 (42.2) | 73 (42.9) | 0.911 |
aData are presented as No. (%).
Table 2.
Age of Hemodialysis Onset in Patients According to Survival Status and Gender a
| Variable | Age of Hemodialysis Onset, y | P Value |
|---|---|---|
| Patients | 0.001 | |
| Alive patients | 54.94 ± 14.3 | |
| Dead patients | 61.75 ± 14.15 | |
| Gender | 0.032 | |
| Male | 57.73 ± 15.22 | |
| Female | 61.63 ± 13.16 |
aData are presented as Mean ± SD.
Table 3.
The Relationship Between BMI, Duration of Hemodialysis and Biochemical Markers in Alive and Dead Patients a
| Variable | Alive Patients | Dead Patients | P Value |
|---|---|---|---|
| Serum Triglyceride, mg/dL | 188.68 ± 92.92 | 181.76 ± 95.11 | 0.575 |
| Serum Cholesterol, mg/dL | 155.38 ± 40.48 | 148.76 ± 40.63 | 0.212 |
| BUN, mg/dL | 152.23 ± 37.19 | 147.94 ± 43.23 | 0.212 |
| Serum Creatinine, mg/dL | 9.44 ± 2.85 | 8.61 ± 3.05 | 0.034 |
| Serum Albumin, gr/dL | 4.16 ± 0.65 | 3.83 ± 0.68 | 0.001 |
| BMI, Kg/m2 | 23.36±4.28 | 28.09 ± 14.85 | 0.654 |
| Duration of hemodialysis, month | 45.82 ± 30.71 | 26.27 ± 23.74 | 0.001 |
aData are presented as Mean ± SD.
| Variable | Gender | P Value | |
|---|---|---|---|
| Male | Female | ||
| Albumin, g/dL | 3.87 ± 0.65 | 4.05 ± 0.72 | 0.044 |
| Triglyceride, mg/dL | 169.48 ± 88.74 | 203.84 ± 98.14 | 0.003 |
| Cholesterol, mg/dL | 143.56 ± 39.31 | 161.11 ± 40.35 | 0.001 |
| BUN, mg/dL | 151.04 ± 43.34 | 147.26 ± 38.27 | 0.465 |
| Creatinine, mg/dL | 9.16 ± 3.19 | 8.54 ± 2.70 | 0.104 |
aAbbreviation: BUN, blood urea nitrogen.
bData are presented as Mean ± SD.
Table 5.
The Influence of the Studied Variables on Mortality a
| Variable | Exp (B) | Sig |
|---|---|---|
| Gender | 1.155 | 0.637 |
| Duration of dialysis | 0.967 | 0.000 |
| BMI | 1.030 | 0.429 |
| Serum albumin | 0.479 | 0.001 |
| Serum Triglyceride | 1.001 | 0.710 |
| Serum cholesterol | 0.992 | 0.051 |
| BUN | 0.999 | 0.732 |
| Serum Creatinine | 0.934 | 0.214 |
aAbbreviation: BUN, blood urea nitrogen.
5. Discussion
Results of the current study demonstrated statistical significant differences between the levels of serum albumin and dialysis duration in patients undergoing hemodialysis. Hypoalbuminemia is the result of the combined effects of inflammation and inadequate protein and caloric intake in patients with chronic disease such as chronic renal failure. Both inflammation and malnutrition reduce albumin concentration by decreasing its rate of synthesis, while inflammation alone is associated with a greater fractional catabolic rate. Hypoalbuminemia is a powerful predictor of mortality in patients with chronic renal failure, and the major cause of death in this population is due to cardiovascular events (8). Many studies demonstrated that a low albumin level is a strong predictor of mortality and morbidity among patients undergoing hemodialysis (9). In a study on 58,058 patients undergoing hemodialysis, the adjusted population-attributable fraction of death due to baseline serum albumin < 3.8 g/dL was estimated 19% (10). Serum albumin predicts all-cause mortality, and peritonitis risk in patients undergoing peritoneal dialysis; however, the data are significantly more limited than those of the patients undergoing hemodialysis (11). In a study by Dutton et al. (12), pre-dialysis albumin appeared to be a poor predictor of nutritional status and did not correlate well with other nutritional parameters. The excess risk of death associated with a low pre-dialysis albumin may be due to fluid overload rather than malnutrition. The results of the current study showed no significant difference between BMI and survival in patients undergoing hemodialysis (P = 0.654). In the general population, there is a significant association between BMI and mortality (13). However, a number of clinical studies have demonstrated that in patients undergoing hemodialysis BMI was inversely related to mortality (14-16). In the United States of America (USA), patients undergoing hemodialysis, a lower BMI is consistently found as a strong predictor of an elevated mortality risk. In contrast, a higher BMI, either overweight or obesity, is generally not associated with any increase in mortality risk, except in Asian Americans. However, only Asian Americans treated with hemodialysis have an elevated relative mortality risk with higher BMI. Outside the US, a higher BMI correlates with a decreased mortality risk (17). One of the hypotheses to explain why low rather than high BMI is associated with an increased mortality risk is the time discrepancies between the competing risk factors (18). A recent analysis in > 300,000 middle-aged adults followed for 15 to 35 years showed that high BMI was associated with increased risks for the development of ESRD as well as mortality (19). In 2004, Johansen et al. (20) performed a large cohort study on 418,055 patients beginning dialysis to investigate the relationship between body size and its outcomes. The results of this study showed that high BMI was not associated with increased mortality among patients beginning dialysis. This finding does not appear to be a function of lean body mass and, although modified by certain patient characteristics, it is a robust finding. The results of the current study indicated no association between serum lipids and survival in patients undergoing hemodialysis. Abnormalities in lipid metabolism occur in patients with all stages CKD (21). In the general population, the serum total cholesterol concentration is clearly a risk factor for coronary disease and death from cardiovascular disease. By comparison, studies on patients with CKD or end-stage renal disease are conflicting: some show a relationship between higher serum cholesterol levels and mortality risk, especially among patients without signs of malnutrition and inflammation (22, 23); some show that low (not high) serum cholesterol values are associated with increased mortality (18, 24); and some show no association between lipid levels and mortality among patients with CKD (25-27). The possibly worse prognosis with low serum cholesterol is thought to reflect the adverse effect of malnutrition and chronic inflammation upon mortality, resulting in a paradoxical reversal risk factor (28, 29). In a study by Iseki et al. (30), dead patients had significantly lower levels of total protein, serum albumin, total cholesterol, triglyceride, BUN, serum creatinine, body weight, body height, diastolic blood pressure, and duration of hemodialysis than those who survived. The results of this study were different compared to those of the current study. In 2010, Herselman et al. (31) performed an exhaustive review and meta-analysis to explore the relationship among serum protein, inflammatory markers, and all-cause and cardiovascular mortalities in adult patients undergoing maintenance hemodialysis. The systematic review included 38 randomized controlled trials (265, 330 patients). They concluded that serum albumin had a significant inverse relationship with all-cause and cardiovascular mortalities, but no significant relationship between pre-albumin and all-cause mortality. C-reactive protein had a significant direct relationship with all-cause mortality, but not with cardiovascular mortality. The potential adverse effects of malnutrition and infections regarding mortality highlight the need for continuous treatment of infections and correction of malnutrition in patients undergoing dialysis. In 2012, Wang et al. (32) performed a meta-analysis to explore the relationship between different BMI ranges and all- cause mortality in patients undergoing hemodialysis. Four studies with totally 81,423 participants met final inclusion criteria. The results of their study showed that the high BMI levels were associated with lower all-cause mortality rate in patients undergoing hemodialysis. More stable hemodynamic status, cytokine and neurohormonal alternations, and nutritional status may contribute to the protective effects of BMI on the mortality of patients undergoing hemodialysis. Among the limitations of the study, it should be noted that it was retrospective, with a small number of patients, without considering admissions, and assessment of the impact of the dialysis technique or doses, although all patients had an adequate dialysis dose. In conclusion, the results of the current study showed that low serum albumin levels and duration of hemodialysis were a strong predictor of mortality and morbidity among patients undergoing hemodialysis.