1. Background
As the elderly population is growing, age-related disorders, such as dementia, are having devastating influences on both families and the society. Dementia is a syndrome with cognitive and non-cognitive dysfunctions, which is represented by memory decline and psychological symptoms (1-3). Beside cognitive impairment, most dementia disorders develop behavioral problems over their course. Depression, aggression, psychosis, night-time behaviors, and behavioral disturbances are repeatedly reported in numerous studies. The prevalence of these symptoms varies due to methodological differences including selection criteria, sampling methods, and study population. Incidence of Behavioral and Psychological Symptoms of Dementia (BPSD) has been reported at about 25% to 80% in patients with Alzheimer’s disease (4-6). Behavioral and Psychological Symptoms of Dementia bring about consequences and high health care costs to both families and the society (4, 7). While psychological and behavioral symptoms are a major domain of dementia, they are not yet considered as an important geriatric health issue in developing countries. Moreover, health professionals do not have experience in the assessment and management of BPSD. Considering the increase in life expectancy in developing communities, there is no doubt that the Behavioral and Psychological Symptoms of Dementia (BPSD) would become a challenging issue in the future. In a study from Turkey, the rate of BPSD was 91.5% with purposeless activity, stealing delusion, and wondering being the most common symptoms (7, 8). In developing countries, multiple families from each generation are used to living together; in this system the ill elderly people are easily cared for by the younger healthy family members. Nevertheless, joint family systems have been fading over the recent years, and consequently, behavioral aspects of dementia are placing substantial and prolonged stress on a given family member such as spouse and children in particular daughters, who do not receive support from the health care systems (9, 10). Many countries in some parts of world are facing the aging of their population. In Argentina with the largest elderly population in Latin America (World bank 2002), a high prevalence of BPSD has been reported in a vast majority of demented subjects (11, 12).
Results of studies in India revealed that the prevalence of BPSD was comparable to the frequency reported from other countries, with, agitation, aggression, and wondering being the common symptoms. Theses symptoms cause an overwhelming burden on care-givers (10, 11, 13).
The most frequent behavioral problems detected by Kaufer et al. were apathy, irritability, and anxiety (11). Considering the severity of dementia, mood symptoms were more prevalent in mild stages of dementia while psychotic features were predominant in moderate to severe stages. In another study investigating the relationship between the caregiver burden and various aspects of dementia, behavioral disturbances, such as aggressiveness, pacing, and shouting, were best predictors of caregiver burden. Likewise, data gathering the prevalence of BPSD and its burden on caregivers in different countries revealed that the behavioral problems were significantly prevalent, and highly overwhelming for caregivers (14-16).
Reviewing studies on BPSD in different countries showed a comparable prevalence of behavioral symptoms in individuals with dementia. However, there is wide discrepancy in the prevalence of most disturbing behaviors across various communities. The difference in reporting challenging behaviors could be due to methodological, ethical, and cultural factors. Some studies exploring behavioral aspects of dementia in the United States and other parts of the world highlighted racial, ethnic, and cultural contribution to the pattern of behavioral symptoms among individuals with dementia (17-19).
In developing countries, cultural, and social values may make family members reluctant to report behavioral and psychological symptoms in their relatives. Moreover, they do not like to give up their social and religious values. Moreover, lack of support groups to help family members, consequently, causes emotional and economical problems for both patients and their families. Therefore, research projects considering the socio cultural background in a particular country are useful to establish an appropriate assessment and management of the behavioral aspects of dementia.
Historically, Iran is still a traditional society with joint families and their own cultural and religious value. They may bring their seniors with dementia to care centers when they are facing behavioral symptoms, which are out of their control.
We designed a cross sectional study to investigate the frequency of behavioral and psychological symptoms in a group of Iranian individuals with dementia. Moreover, we aimed to detect potential sociodemographic and clinical contributing factors.
2. Methods
2.1. Samling
This study had a cross sectional designe and was conducted at a university psychogeriatric outpatient clinic, in Shiraz, Iran, during year 2014.
With a convenient sampling method, 131 dementia outpatients aged over 50 years old were selected. Patients were excluded if their companies were reluctant to participate or were not the main caregiver of the patients. Overall, 30 patients were excluded and 101 subjects were left for analysis. This study was approved by the ethics committee of the research deputy of the university.
2.2. Measures
2.2.1. Neuropsychiatry Inventory
Cognitive status and behavioral disturbance were assessed by the Neuropsychiatric Inventory (NPI). The NPI involved the following 13 items, dellusion, hallucination, agitation, apathy, anxiety, depression, euphoria, irritability, disinhibition, aberrant motor behavior, change in appetite, and night time behavior disturbances, which were gathered from main family caregivers spending most of their time with the patient. Rating on the frequency and severity of the behavior were made by the care giver on the basis of administered questionnaires, and calculation of average scores. The severity was ratified to 1 = mild, 2 = moderate, and 3 = severe; frequency was rated as 1 = occasionally, 2 = often, 3 = frequently, and 4 = very frequently. The total scores of the individual subscales for global score of the NPI was then summed up (20).
2.2.2. Barthel Index
The Barthel index was utilized to measure the degree of the patient’s dependence on the care giver for daily tasks (10 tasks); feeding (0 = unable, 5 = needs help, and 10 = independent), bathing (0 = dependent and 5 = independent), grooming (0 = needs help and 5 = independent), dressing (0 = dependent, 5 = needs help, but, can do about half unaided, and 10 = independent), bowels (0 = incontinent, 5 = occasional accident, and 10 = continent), bladder (0 = incontinent, 5 = occasional accident, and 10 = continent), toilet use (0 = dependent, 5 = needs some help, and 10 = independent), transfers (0 = unable, 5 = major help, 10 = minor help, and 15 = independent), mobility (0 = immobile, 5 = wheelchair independent, 10 = walk with help of one person, and 15 = independent), and stairs (0 = unable, 5 = needs help, and 10 = independent) (21).
2.2.3. Cumulative Illness Rating Scale (CIRS)
Burden of comorbid medical conditions was assessed by the Cumulative Illness Rating Scale (CIRS) (22).
2.2.4. Clinical Dementia Rating (CDR) Scale
Severity of dementia was evaluated by the Clinical Dementia Rating (CDR) scale (23).
2.3. Statistical Analysis
Statistical analysis was performed with the SPSS (version 21) software.
The psychometric of the NPI was studied with several approaches. The t-test was determined to assess associations between total NPI patient distress and total NPI care giver distress with clinical dementia rating. Also t test was used to assess the association between types of dementia with total NPI patient distress. Pearson correlation was calculated for total NPI patient distress and total NPI care giver distress scores. The Analysis of Variance (ANOVA) assesses the association between CDR and NPI delusion of patients. Also Kruskal Wallis assessed the association between CDR and Barthel Index.
3. Results
In this study, 101 patients including 44 females (44%) and 56 males (56%) with mean age of 78.3 (SD ± 8.4) were included. Details of demographic characteristics of patients are listed in Table 1.
Table 1. Clinical and Demographic Characteristics of the Study Sample
| Variable | N (Percentage) | |
|---|---|---|
| Gender | Female | 44 (44) |
| Male | 57 (56) | |
| Maritalstatus | Married | 56 (55) |
| Widowed | 39 (39) | |
| Other | 6 (6) | |
| Education | Illiterate | 59 (58) |
| Primary (< 12) | 12 (12) | |
| Diploma (= 12) | 16 (16) | |
| Above diploma (> 12) | 14 (14) | |
| Livingarea | Urban | 74 (73) |
| Rural | 27 (27) | |
| Caregiver | Spouse | 38 (38) |
| Children | 58 (57) | |
| Career | 5 (5) | |
| Job | Unemployed | 76 (75.3) |
| Retired | 23 (22.8) | |
| Employed | 2 (1.9) |
Using Diagnostic and Statistical Manual of Mental Disorders, 4th Edition (DSM IV) criteria, patients were allocated to 5 major groups, including 76 Alzheimer’s dementia (75%), 19 vascular dementia (19%), 3 frontotemporal dementia (3%), 3 lewy body dementia (3%), and others (0). Considering the severity of dementia, patients were categorised in four groups; 15 severe (14.9%), 39 moderate (38.6%), 34 mild (33.7%), and 13 undetectable (12.9%).
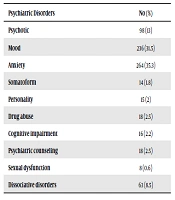
Further analyses exploring prevalence and type of behavioral problems revealed a wide range from 5% for elation to 69% for night time behaviors. The most common problematic behaviors were night time behaviors followed by delusion (58%), disinhibition (57%), anxiety (57%), irritability (56%), depression (55%), agitation (55%), and apathy (55%). Although, psychological symptoms such as eating behavior, aberrant motor behavior, and hallucination were not as high as the above symptoms, they were still significantly prevalent (Table 2).
Table 2. Neuro Psychiatric Inventory Scoring Summary
| No. (%) | |
|---|---|
| Delusion | 59 (58.4) |
| Hallucination | 44 (43.6) |
| Agitation | 55 (54.5) |
| Depression | 56 (55.4) |
| Anxiety | 58 (57.4) |
| Elation | 5 (5) |
| Apathy | 56 (55.4) |
| Disinhibition | 58 (57.4) |
| Irritability | 57 (56.4) |
| A.M.B | 31 (30.7) |
| Insomnia | 70 (69.3) |
| Appetite | 32 (31.7) |
Abbreviation: A.M.B, aberrant motor behavior
Increase in behavioral problems led to higher distress in caregivers. Night-time behaviors were the most distressful problems, which were significantly correlated to care giver distress (r = 0.85 and P value = 0.001). Delusion, hallucination, irritability, disinhibition, and aggression were other symptoms, which caused more trouble for patients and their caregivers. The level of distress perceived by both patients and caregivers were significantly associated (P = 0.001), so that the higher patient distress predicted higher caregiver distress (Figure 1).
 Patient Distress and Total NPI Care Giver Distress")
Figure 1.
Correlation Between Total Neuropsychiatry Inventory (NPI) Patient Distress and Total NPI Care Giver Distress
The prevalence of behavioral and psychological symptoms and level of distress were significantly correlated to the severity of dementia. As the stage of dementia increased, the level of distress increased in both patients and their caregivers. In our analyses, NPI total patient distress (P value = 0.001) and NPI total caregiver distress (P value = 0.001) were significantly associated with the CDR score.
Delusion (P = 0.006), hallucination (P = 0.006), aggression (P = 0.003), apathy (P = 0.001), disinhibition (P = 0.001), irritability (P = 0.001), aberrant motor behaviors (P = 0.004), sleep problems (P = 0.001), and eating behaviors (P = 0.02) were positively associated with the CDR score. However, prevalence of depression (P = 0.09), anxiety (P = 0.3), and elation (P = 0.2) were not increased with the severity of dementia.
Because of the small sample size, patients were allocated to Alzheimer’s (76) and non-Alzheimer’s (24) groups. In patients with non-Alzheimer’s dementia, higher total NPI patient distress was detected (P value = 0.001) while total NPI caregiver distress was higher in the non-Alzheimer’s group (P value = 0.03).
In this study mean Barthel index was 69.45 ± 27.86, which had a significant association with CDR (P value = 0.001). Likewise CDR was significantly associated with CIRS scores; higher cumulative illness burden was detected at more severe stages of dementia (P value = 0.001).
Detailed analyses did not detect any association between severity of dementia and frequency, and type of behavioral and psychological symptoms with demographic factors such as marital status, living area, caregiver, and education.
4. Discussion
Data from the current study revealed that most of the behavioral problems detected by the Neuropsychiatry Inventory (NPI) were significantly prevalent among a group of Iranian elderly with dementia. Night-time behavior with a prevalence of 69% was the most common symptom followed by delusion, disinhibition, anxiety, irritability, depression, agitation, and apathy. Other psychological symptoms such as eating behavior, aberrant motor behavior, and hallucination were not as high as the above symptoms, yet, they were still significantly prevalent. The only symptom, which was less reported was elation.
The findings of this study suggested that the three main cluster symptoms were psychosis, behavioral disturbances such as disinhibition and irritability agitation, and mood symptoms, including anxiety and depression. Interestingly, regardless of methodological, cultural and racial variability, these findings have been replicated by earlier published literature. In one study in Japan, higher rate of positive symptoms, such as delusion and aberrant motor behaviors, were found in Alzheimer’s disease (25).
Similar to the present study, the association between these problematic behaviors and severity of dementia was replicated by earlier studies as well (7, 10, 11, 14-17, 19, 24, 26, 27). For instance, in some previous studies, sleep problems, irritability, agitation, aggression, and psychosis were among the most disturbing behaviors reported by caregivers, which were predominantly associated with the severity of dementia (11, 14, 16, 19). Inconsistent with these studies in a study from Korea, BPSD were fairly common in very mild Alzheimer’s dementia (1). Also, in this study dementia severity and its subsequent behaviors were correlated with higher care-giver distress. This finding has been reported by other studies, which found strong a correlation between neuropsychiatry symptoms and total care giver distress score. Similarly, some sub-items of NPI, like night-time behavior, caused distress to both patients and care-givers (14, 16, 28).
On the other hand, in line with earlier cross cultural studies, mood symptoms, such as depression and anxiety, were more predominant at earlier stages of cognitive impairment than later stages (11, 19, 27). The more common emotional problems in early stages of dementia might be due to the preserved insight at the early stage when patients can emotionally react to their cognitive decline. Moreover, detecting emotional symptoms at later stages needs more specific instruments. High level of anxiety and depression while cognitive failure has still not set in could lead to misdiagnosis.
Another finding of this study was that cumulative burden of medical illnesses was associated with the severity of dementia and its subsequent problematic behaviors. In this study, the most common comorbid medical conditions were disorders related to hearing and vision followed by vascular disorders and musculoskeletal problems.
The level of disability in activities of daily living was positively associated with the stage of the dementia, frequency of psychological and behavioral symptoms, and distressed perceived by the caregivers. Although patients with non-Alzheimer’s dementia were younger than the Alzheimer’s group, they still showed higher level of disability. This finding supports the idea that the disability is mostly related to the dementia process rather than ageing. Greater medical comorbidity and the pathological nature of non-Alzheimer’s type, such as vascular pathology, could lead to a more disabling course than Alzheimer’s dementia.
We did not detect any association between severity of dementia and frequency, and type of behavioral and psychological symptoms with demographic factors such as marital status, living area, caregiver, and education. The report form studies considering various communities have not been conclusive (12, 13, 15, 17).
However, the small sample size might be a limitation to come out with a conclusion. Additionally, this study was conducted at a psychiatry clinic where families present their elderly when they have problematic behaviors. In the same report, which included a large number of patients with Alzheimer’s dementia, vascular dementia, and diffuse levy body dementia, incidence and characteristics of neuropsychiatric symptoms suggested that researchers have been mainly concerned with abnormal behaviors of advanced dementia patients (29).
While the symptom profile among our sample was not exactly the same as BPSD reported by other studies, the type and frequency of symptoms were still similar. Data from this study and other studies have not been suggestive of a particular cultural and ethnical factor contributing to type and prevalence of BPSD. Even those studies comparing various communities have not been conclusive (15, 27, 30). Cultural and social values may encourage caregivers to under-report BPSD in their senior relatives and patients with dementia are brought about when their behavior bothers themselves and their caregivers.
Discrepancy between type and prevalence of psychological and behavioral problems reported from different countries could be due to terminology and methodological issues. For instance, the instruments detecting the psychological and behavioral problems have not been the same in published literatures; BEHAVE-AD (8, 10, 30) and NPI were used in different studies (11).
The current life expectancy in Iran is 70, and 7% of the population are older than 60, which is growing rapidly. General practitioners and even general psychiatrists and neurologists do not have enough experience in detecting and managing BPSD. Like other developing countries, Iranian families, in particular their spouse and children are the main caregivers of their elderly (31). Meanwhile, multiple family patterns have been changing, which could place the burden of care giving for elderly on one or two relatives, mostly their spouses.
It would be reasonable to institute strategies that would raise awareness of health professionals and family caregivers about BPSD. Development of Cheap and feasible education and training interventions in BPSD could ameliorate patient behaviors, improve activity of daily living, and reduce caregivers’ distress. Further studies focused on pharmacological and easy available psychosocial interventions with a probable wide usage in developing countries like Iran would improve the management of BPSD at home.