




1. Introduction
Oral focal mucinosis (OFM) is an uncommon tumor-like growth of unknown etiology, and is the oral counterpart of cutaneous focal mucinosis (1, 2). The occurrence of oral lesions was first mentioned by Tomich in 1974. The study proposed that OFM develops due to local hyaluronic acid overproduction by fibroblasts (3). OFM commonly occurs during the fourth and fifth decades of life (2). OFM is more common in women and most commonly found on the gingiva (2, 4). Clinically, OFM appears as a solitary, painless, non-ulcerated, round, elevated overgrowth with a similar color to the surrounding normal mucosa. The histopathological features of OFM are characterized by the presence of myxomatous degeneration of connective tissue stroma, mostly of keratinized mucosa overlying the alveolar bone. The myxomatous degeneration occurs due to the overproduction of hyaluronic acid by the fibroblasts in the connective tissue, at the cost of collagen production (5). Its treatment involves complete surgical excision, and no case of recurrence is known (6). The present study evaluated the clinical signs, histopathology, and treatment of oral focal mucinosis in the gingiva around the dental area of 44 and 45 in a 53-year-old female patient.
2. Case Presentation
A 53-year-old female patient presented to the Dental University of Babol, complaining of an asymptomatic swelling on her gingiva around the dental area of 44 and 45 starting three months ago. The patient had systemic hypertension and she was taking losartan. The intraoral examination revealed a 1×1 cm light red, elastic, painless, sessile lesion, and the overlying mucosa was non-ulcerated in the gingiva around the dental area of 44 and 45. The patient had poor oral hygiene. The differential diagnosis of peripheral giant cell granuloma and pyogenic granuloma was established.
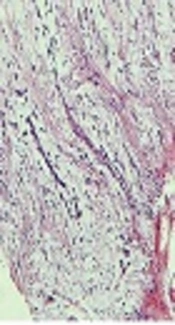
The lesion was excised surgically (excisional biopsy) under local anesthesia and histopathologically evaluated. The H&E stained microscopic slide showed the parakeratinized hyperplastic stratified squamous epithelium with a loose underlying myxomatous stroma, with oval, fusiform, and stellate-shaped fibroblasts (Figures 1 and 2). Based on these histological findings, the diagnosis of OFM was established.
")
Figure 1.
The parakeratinized hyperplastic stratified squamous epithelium with underlying loose and myxomatous stroma (hematoxylin and eosin staining × 10)
")
Figure 2.
Loose and myxomatous stroma, with oval, fusiform, and stellate-shaped fibroblasts (hematoxylin and eosin staining × 10)
3. Discussion
OFM is a rare clinicopathological condition and is the microscopic counterpart of the cutaneous focal mucinosis. In 1966, Johnson and Helwig explained solitary, asymptomatic, white papules or nodules usually seen on the face, trunk, and extremities, naming them as cutaneous focal mucinosis (7). OFM was first mentioned by Tomich in 1974 (3). The gingiva is the most common site for OFM (8). Its pathogenesis can be the result of the overproduction of hyaluronic acid by fibroblasts, which results in the degeneration of the connective tissue (9). OFM has no distinct clinical characteristics and it is often clinically considered as mucocele, pyogenic granuloma, fibroma, or similar lesions (10). Safer et al. proposed that most of these lesions represent a myxomatous or “mucinous” change in a preexisting fibrous lesion (9, 11). Histopathologically, OFM must be differentiated from nerve sheath myxoma and peripheral odontogenic myxoma. The nerve sheath myxoma is a more restricted nodule separated by fibrous septa, and its stromal cells are plumper. Peripheral odontogenic myxoma displays the presence of mast cells, increased reticular fibers, and islands of odontogenic epithelium (11, 12). Since the first report of OFM, nearly 57 cases have been recorded, with only one recurrence case in a 25-year-old woman reported by Narayana and Casey (2). Soda et al. in 1998 reported an interesting case of OFM in the ventral tongue (13). A review of all reported cases indicated that OFM has never been clinically diagnosed (14). Histological studies play a significant role in the accurate diagnosis of OFM, including loose and myxomatosis stroma with stellate-shaped fibroblasts, with or without inflammation (10, 14-16). OFM stains positive with alcian blue, indicating the abundant mucins scattered around the connective tissue (3, 10, 15, 17). Its treatment involves complete surgical excision, and no recurrence is reported (10, 16, 18). In the present case report, the excisional biopsy was performed.
3.1. Conclusions
In the clinical examination of the recent case, the lesion was similar to irritation fibroma. It is worth mentioning that a preoperative diagnosis is almost impossible in many lesions because of their rarity. Therefore, the histological evaluation is always the basis for the diagnosis of OFM.

