1. Background
Violence in the workplace is one of the most common occupational hazards in health systems worldwide (1-3). Violence in the workplace refers to the occurrence of angry behavior and physical or verbal aggression by others (4). Violence is the act of any form of physical, sexual, verbal, racial, or occupational violence or intimidation in the workplace that may result in actual or potential harm to one's health (5). According to the WHO statistics, about 8% to 38% of hospital personnel are exposed to violence, especially physical ones (5).
There are different types of violence in the workplace, which are divided into four categories: Verbal, physical, cultural-racial, and sexual violence (6). Although violence occurs in all workplaces, health care workers are more prone to violence (4). It has been found that 65% of older nurses are exposed to violence. Studies have also shown that 60% to 90% of nurses experience verbal or physical violence during their working period (7). The main reason for the prevalence of violence against nurses is their close contact with patients and their companions and the responsibility of caring for patients in situations threatening their health (8). In addition, many nurses have been abused by their co-workers and superiors during their hospital work hours. A systematic study reported that despite the cultural diversity in different countries, nurses' response to violence includes anger, fear, anxiety, self-blame, guilt, PTSD signs and symptoms, and shame. These symptoms can persist long and change nurses' social life, mental health, and perceptions of their profession (9). In addition, violence can be an obstacle to patient care and cause leaving the job (10-13).
The COVID-19 disease has been declared a pandemic (14), and facing this critical situation for nurses and medical staff who are at the frontline of treatment, diagnosis, and care of COVID-19 patients is very stressful, leading to a variety of problems and mental disorders (15). In addition, this disease leads to a lot of stress and anxiety for medical staff, patients, their families, and nurses and doctors who are in charge of patients' health and have the most contact with the patients and their families (16-18). The increasing number of COVID-19 cases, overwork, shortage of medical and protective equipment, lack of access to special drugs, and media coverage of this disease can impose a psychological burden and lead to high stress for medical staff, including nurses (15). Also, fear of getting sick and communicating with patients has caused numerous verbal or physical violence. Some studies found that nurses suffered much violence in the workplace during the COVID-19 pandemic (19-21). Also, according to a study in Iran, nurses suffered different kinds of violence during the COVID-19 pandemic (22). Also, based on the conducted studies, there is little related evidence so far in this regard.
2. Objectives
The present study aimed to investigate violence against nurses at the Razi educational and remedial center in Rasht.
3. Methods
3.1. Participants and Study Design
This cross-sectional study was performed on 112 nurses working in the emergency departments of Razi hospital in Rasht, one of the referral centers for COVID-19 patients in Rasht, selected by a convenience sampling method in August 2020. Inclusion criteria were having at least one year of work experience, a bachelor's degree, and direct contact with COVID-19 patients. Exclusion criteria were nurses suffering from mental illnesses such as depression, incomplete questionnaires, and nurses' unwillingness to participate.
The sample size was determined with 95% confidence and based on the study of Dehnabi et al. (23). With a 10% attrition rate, the total sample size was determined to be 112 people.
3.2. Ethical Considerations
This study was approved by the Guilan University of Medical Sciences Ethics Committee (ethics code: IR.GUMS.REC.1399.024). All nurses were informed of the research's objectives and the confidentiality of data. Also, they were assured that their information would be used for study purposes only, and informed consent was received from all participants before completing the questionnaires.
3.3. Data Collection
A questionnaire on violence against nurses was used to assess violence against nurses by patients, their families, supervisors, and colleagues. This questionnaire is a modified version of the World Health Organization questionnaire in the field of workplace violence in health settings, which has been psychometrically assessed by Najafi (6) in Iran. The questionnaire's validity and reliability have been approved in several Iranian studies. This questionnaire has three parts. The first part includes 18 questions to survey nurses' demographic characteristics and questions about nurses' views on factors predisposing to violence, the most important reasons for not reporting violence, and the most important reason for violence. The second part includes 18 questions about the prevalence of various types of violence (verbal, physical, cultural-racial, and sexual) by the patients, their families, supervisors, and colleagues at work. Each item is answered as "every week," "every month," "every 2 - 3 months", and "never." The perpetrators of violence are also categorized as "patients," "patient family", “colleagues,” and “matron and supervisor.” The third part is about the response and actions of nurses to violence in the workplace (with yes/no answers). Completion of this questionnaire was not time-consuming, and the average time for completing this questionnaire was 15 minutes.
3.4. Statistical Analysis
After collecting data and entering it into SPSS version 22 software, the data normality was measured with the Kolmogorov-Smirnov test and statistical tests, including chi-square, independent t test, and Fisher's exact test. The significance level of the tests was considered less than 0.05.
4. Results
Out of 120 distributed questionnaires, eight were not completed by nurses, and as a result, 112 nurses were included in the study. Most were women (94%), their mean age was 33.11 ± 5.22 years, and most were married (78%). Most (65%) had governmental employment, with an average work experience of 4.55 ± 5.26 years. The majority had a bachelor's degree in nursing (97%) and served as a nurse with shift rotation (96%). Most were full-time (91%) and in direct contact with patients (98.5%). Verbal violence was the most common type against nurses during the last six months, 62.5% (n = 70), which was applied by patients (55%) for most nurses. The frequency of physical violence was 17.8% (n = 20) that mostly occurred by the patients’ family in 67% (n = 50), followed by patients in 67% (n = 50), physicians in 6.2% (n = 7), other nurse colleagues in 5.3% (n = 5), head nurses in 4.4% (n = 4), and other people in 2.6% (n = 3). No sexual or racial (cultural) violence was reported.
The highest frequency of violence was physical and occurred during the night shift (38.2%) and verbal violence in the evening shift (44%). In most cases, the male gender committed both types of violence [verbal violence (88%) and physical violence (77%)].
Concerning the reactions, most nurses invited the attacker to calm down (62.5%). According to nurses’ responses, 37.5% (n = 42) mentioned that the uselessness of reporting was the most common reason for not reporting violence in the hospital. The other reasons were shyness (n = 12; 10.7%), fear of bad consequences (n = 8; 7.1%), and blame themselves (n = 5; 4.45%).
Also, there was no significant relationship between age and work experience in the emergency department and the frequency of verbal and physical violence. There was a significant relationship between education level and the frequency of verbal violence (P = 0.02).
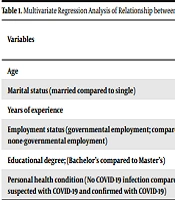
Linear regression analysis showed that nurses with low experience were 1.01 times more likely to undergo violence (OR = 1.01; CI: 0.66 - 1.44) (Tables 1 and 2).
Table 1.
Multivariate Regression Analysis of Relationship Between Independent Variables and Physical Violence Against Nurses
| Variables | Non-adjusted (Simple) | Adjusted (Multiple) | ||||||
|---|---|---|---|---|---|---|---|---|
| B a | β b | CI 95% | P | B a | β b | CI 95% | P | |
| Age | 8.09 | 0.56 | 1.17 (0.75 - 1.85) | 0.55 | 3.06 | 0.44 | 0.67 (0.22 - 2.2) | 0.66 |
| Marital status (married compared to single) | 9.01 | 0.45 | 0.77 (0.55 - 1.1) | 0.12 | 7.09 | 0.31 | 1.02 (0.6 - 2.01) | 0.71 |
| Years of experience | 7.99 | 0.87 | 1.01 (0.66 - 1.44) | 0.08 | 8.89 | 0.63 | 2.1 (0.45 - 0.77) | 0.04 c |
| Employment status (governmental employment; compared to none-governmental employment) | 9.98 | 0.54 | 0.71 (0.44 - 1.8) | 0.51 | 9.97 | 0.66 | 0.71 (0.44 - 1.57) | 0.31 |
| Educational degree; (Bachelor’s compared to Master’s) | 1.78 | 0.65 | 0.61 (0.44 - 1.11) | 0.64 | -6.09 | 0.56 | 0.64 (0.44 - 2.08) | 0.59 |
| Personal health condition (no COVID-19 infection compared to suspected with COVID-19 and confirmed with COVID-19) | -1.69 | 0.44 | 0.71 (0.31 - 2.11) | 0.001 | -1.89 | 0.57 | 1.87 (1.03 - 2.055) | 0.64 |
Abbreviation: CI, confidence intervals.
a Unstandardized regression coefficients.
b Standardized regression coefficients as beta.
c Statistically significant at P < 0.05.
Table 2.
Multivariate Regression Analysis of Relationship Between Independent Variables and Verbal Violence Against Nurses a
| Variables | Non-adjusted (Simple) | Adjusted (Multiple) | ||||||
|---|---|---|---|---|---|---|---|---|
| B a | β b | CI 95% | P | B a | β b | CI 95% | P | |
| Age | 9.11 | 0.55 | 2.02 (0.67 - 1.78) | 0.67 | 2.89 | 0.63 | 0.49 (0.69 - 2.9) | 0.78 |
| Marital status (married compared to single) | 1.08 | 0.44 | 1.07 (0.45 - 1.6) | 0.76 | 6.98 | 0.44 | 3.56 (0.9 - 2.49) | 0.76 |
| Years of experience | 8.99 | 0.78 | 1.6 (0.65 - 1.45) | 0.78 | 7.45 | 0.68 | 4.6 (0.56 - 0.78) | 0.67 |
| Employment status (governmental employment; compared to none-governmental employment) | 8.79 | 0.66 | 0.49 (0.34 - 1.7) | 0.59 | 9.77 | 0.69 | 0.44 (0.12 - 1.89) | 0.53 |
| Educational degree (Bachelor’s compared to Master’s) | 1.77 | 0.64 | 0.78 (0.58 - 1.8) | 0.08 | -6.89 | 0.55 | 0.88 (0.34 - 2.12) | 0.04 c |
| Personal health condition (no COVID-19 infection compared to suspected with COVID-19 and confirmed with COVID-19) | -1.80 | 0.45 | 0.89 (0.55 - 2.67) | 0.97 | -1.68 | 0.53 | 1.69 (1.13 - 2.08) | 0.67 |
Abbreviation: CI, confidence intervals.
a Unstandardized regression coefficients.
b Standardized regression coefficients as beta.
c Statistically significant at P < 0.05.
5. Discussion
This study showed a high level of violence against nurses in the Razi educational and remedial center in Rasht. Regarding physical violence, a study conducted in East Azerbaijan also showed a high level of violence (24). Shoghi et al., in their study on violence among nurses working in 20 hospitals in Tehran, showed that 19.1% of nurses had been subjected to physical violence at least once in the last six months (25). Senuzun Ergun and Karadakovan reported 19.7% of physical violence in Turkey (26). Shields and Wilkins reported a 34% incidence of physical violence in their study in Canada (27). However, Nachreiner et al. estimated 13.2% yearly physical violence (28).
Violence against nurses can occur for various reasons, such as direct and more contact of nurses with patients and their companions, lack of facilities, and high workloads. In many cases, due to the nurse being at the forefront of care, the patients and families consider her the leading cause of possible deficiencies and thus resort to violence. Regarding the shifts in which violence occurred, the present findings showed that the exposure to physical violence was higher in the night shift. In a study in Canada, Shields and Wilkins reported that physical violence was most prevalent in the evening shift (40.2%), followed by the night shift (38.7%) (27). Estryn-Behar et al. also found a significant relationship between night shift and violence (29). The higher level of violence during night shifts can be due to the shortage of security forces or workforce, including doctors and nurses, or even equipment. The perpetrator of physical violence in the present study was the patient in most cases, and the gender of the perpetrator of physical violence was male in most cases. Farrel et al. reported that the patients were the most common perpetrators of physical violence in Australia (30). In another study in the emergency department of a hospital in Tehran, Hasani et al. stated that in most cases, physical violence was committed by the patient and patient family, and most perpetrators of violence were men (31). Many studies have shown that the expression of violence is higher in men than in women. In addition to the high stress and anxiety that patients and their families experience during hospitalization, which can result in violence, some injuries such as head injuries, severe limb disease, glucose deficiency, and incurable diseases can cause violence (32).
Regarding verbal violence, the present study showed that the majority of them were subjected to verbal violence during their work at the hospital. Talas et al. reported verbal violence in Turkish nurses in 79.6% of cases (33). However, the rate of verbal violence in the study by Zamanzadeh et al. was 72.1% in East Azerbaijan hospitals (24). The present study showed that verbal violence occurred in most cases during the evening shift. Salimi et al. reported that verbal violence mainly was reported during the evening and night shifts (34). In this study, the perpetrator of verbal violence in most cases was the patient family, followed by the patient. In another study in Ankara, Talas et al. reported that the level of verbal violence was 98.8% by the patient family and 64.2% by the patients (33). Violence in less crowded shifts, such as evening and night shifts, can be associated with the shortage of nurses in the hospital.
Regarding the frequency of reported and unreported cases of physical and verbal violence and their causes, the findings showed that most participants acknowledged that they reported a high level of violence, while Shoghi et al. showed the rate of reporting violence was only 35.9% (25). In another study, Senuzun Ergun and Karadakovan stated that the rate of non-reporting violence was 62.9% (26). Kitaneh and Hamdan in Palestine reported a 56.3% rate of non-reporting violence (35). Our results showed that most nurses believed reporting violence was useless, and some considered its occurrence unimportant. They did not consider it part of their profession, which may be due to nurses' lack of familiarity with their individual, social, and professional rights. They believe that violence by patients, their families, or colleagues is part of their job, and nurses' experience of inappropriate action by managers to whom violence had been reported or even their indifference causes the abused nurse to avoid reporting it. In this regard, Kitaneh and Hamdan also state that nurses were ashamed of reporting violence and were worried about their future careers, and some did not consider the occurrence of violence as important and did not report it (35).
However, Zamanzadeh et al. stated that non-reporting violence and consequently the shortage of information in this field is one of the main problems in implementing programs to reduce violence. Also, the lack of instructions on reporting violence or the complexity and time-consuming reporting process can be another factor in non-reporting the violence. However, failure to report violence prevents appropriate action against it (24). All these factors can be influential in not reporting the violence, but the authorities' lack of accurate and proper tracking can play a significant role. In examining the relationship between verbal and physical violence and individual and social variables, we found a significant relationship between nurses’ education levels and verbal violence. Mohamed's study observed a significant relationship between violence and education level (36). In another study, these two variables had a statistically significant relationship (37). Perhaps raising the level of education by increasing public awareness and culture could affect the incidence of violence.
According to linear regression analysis, nurses with low experience were 1.01 times more likely to undergo violence (OR = 1.01; CI: 0.66 - 1.44). In this regard, a study by Kitaneh and Hamdan reported a significant relationship between nurses’ experience and violence (35).
5.1. Limitations
In the present study, sampling was performed only in one central hospital for COVID-19 in Guilan province, and it may not be possible to generalize the results to all nurses in Guilan province of Iran. Therefore, further research in this field is recommended.
5.2. Conclusions
The results showed a significant rate of physical and verbal violence against nurses working in the Razi educational and remedial center in Rasht. Establishing a process for reporting violence and providing organizational support to affected nurses can help report the violence. In addition, some policies are proposed to reduce and prevent violence in the workplace, such as increasing human resources, reducing the workload of nurses, training novice nurses to have communication skills and control violence, providing a safe work environment, supporting employees, providing isolation and containment rooms for aggressive patients, counseling and reporting violence against the victim nurse, providing a coherent process to track and report the violence, and providing psychological care for the victim nurse.