


1. Introduction
Syphilis is a sexually transmitted disease caused by the bacterium Treponema pallidum. Syphilis can cause serious health effects without adequate treatment.
Some so-called "rare" clinical presentations in syphilis pose a real diagnostic challenge; sometimes, this diagnosis can be missed or delayed with delayed therapeutic management. Although most physicians think to include syphilis in the differential diagnosis of a wide range of symptoms, some presentations may surprise even the most experienced clinicians.
Myositis is an inflammation of striated muscle tissue. Among its causes, autoimmune conditions are the main ones. However, infectious causes are also incriminated, such as Coxsackie B virus epidemic myositis (1). Treponemal myositis or syphilitic myositis is, however, exceptional. Its localization or predominance on the facial muscles is even rarer. We report the case of a facial form of syphilitic myositis with a study of the clinical and radiological characteristics. To our knowledge, this myositis manifestation and its facial localization have never been reported.
2. Case Presentation
A patient aged 25 years of Malian origin presented to the Neurology Department of Mustapha Bacha University Hospital with a painful facial diplegia. The neurological picture of sub-acute onset was marked by a reduction or even abolition of facial mimicry, with the impossibility of whistling, blowing, or even smiling. The closure of the eyes was partial when falling asleep. This picture was completed after a few days of pain that felt like cramps, especially when palpating his face. He did not report any previous dermatological lesions or adenopathy. The neurological examination revealed facial diplegia with Charles Bell's sign on both sides, an inability to smile, and paralytic dysarthria. There were no swallowing or phonation disorders. Nausea and soft tissue reflexes were present. The rest of the neurological examination was normal (Figure 1).

Facial diplegia
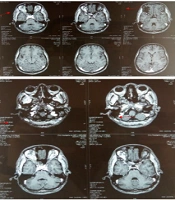
Brain and facial MRI showed diffuse thickening of the Temporalis muscles bilaterally, the internal and external pterygoid muscles, and the paraspinal and long neck muscles, with heterogeneous enhancement after injection of the contrast medium (Figure 2).

Facial and cerebral MRI
The inflammatory panel was disturbed with positive CRP with a rate of 34 and accelerated sedimentation rate (35/80). Muscle enzymes were normal. A lumbar puncture showed medium cellularity (55 elements) with a predominance of leukocytes, and syphilitic serology was positive. HIV serology was requested, but no result was obtained. The patient was referred to the infectious diseases department for treatment.
3. Discussion
In syphilis, direct skeletal muscle involvement is uncommon, although several case reports have appeared in the literature (1). In the primary and secondary stages of the disease, generalized myalgia is a common symptom, but its presentation as an inflammatory myopathy is rare. The first case was reported in 1965 by Towpik and Mrozek (2) and involved the limb belts. Only 2 other cases were subsequently published, in 2010 and 2011, but only involved the musculature of the limbs, never the face (3, 4). Involvement of the facial muscles has never been reported, making our case the first reported case of inflammatory involvement of the facial muscles of syphilitic origin with suggestive imaging. Our patient's bilateral facial myopathy mimicked facial diplegia. It is, therefore, advisable to consider facial syphilitic myositis in any subject presenting with this symptomatology. Syphilis, in its myositic form, has rarely been evoked, and this patient bears witness to the fact that the resurgence of this condition can manifest itself in atypical disorders of neurological order other than those already identified in the literature.
3.1. Conclusions
Although myalgia is commonly seen in primary or secondary syphilis, inflammation of muscle tissue is not. Our "anecdotal" case confirms that syphilis should be considered when faced with myositis of uncertain etiology and that facial muscle involvement can be confusing as it is exceptional. However, imaging and infectious work-up can point to the correct diagnosis.
